Introduction
Kinesiology tape is widely used by health professionals to manage musculoskeletal conditions because of its cost effectiveness, ease of application, and accessibility,1 but the use of kinesiology tape for respiratory management in adults is inconsistent. Some studies report positive clinical effects,2–4 while others report no significant benefits.5,6 When applied to respiratory muscles such as the diaphragm, kinesiology tape may improve proprioceptive awareness, posture, promote ventilation, and deeper inspiration, potentially increasing lung volumes in both healthy adults and individuals with chronic obstructive pulmonary disease (COPD), with a subsequent increase of lung volumes.3,5,7–9 Additionally, accessory respiratory muscle taping, which includes applying kinesiology tape along the intercostal or scalene muscle fibers with light tension (20-30%) from origin to insertion, may also facilitate inspiratory activation.4
Physiotherapy interventions such as deep breathing exercises (DBE), and inspiratory muscle training (IMT) aim to maintain or restore respiratory function.7,10,11 Some modalities, including mechanical insufflation-exsufflation, are costly and require specific skill.12 In contrast, techniques such as DBE,13 and blow bottles14 are affordable, and some authors have suggested that kinesiology tape could offer potential benefits.1 In middle- and low-income countries, affordable interventions are needed to improve respiratory function in adults.
Although systematic reviews have primarily focused on kinesiology taping in sports, musculoskeletal conditions,15–17 oncologic and internal organ conditions,18 its efficacy specifically for respiratory conditions remains unverified.9 This paper reviews the literature examining the efficacy of kinesiology tape in healthy adults and individuals with respiratory conditions, as part of a larger systematic review including neurological conditions.
Methods
This systematic review followed the Cochrane methodology and PRISMA guidelines, was registered with PROSPERO (CRD42023390690), and received institutional ethics approval (629/2022).
Data sources and literature
Eight electronic databases (Academic Search Complete; Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature, Medline, Physiotherapy Evidence Database, PubMed, Science Direct, and Scopus), a search engine (Google Scholar; from 2013 - 2023), grey literature, and reference lists of included studies were searched from inception until April 2023, using keywords (Medical Subject Headings: https://www.ncbi.nlm.nih.gov/mesh/) based on the PICOS (Population, Intervention, Comparison, Outcome measures and Study design) framework.
Primary and secondary outcomes
The primary outcomes included the effects of kinesiology tape on respiratory function among healthy adults and adults with respiratory conditions. Outcomes included lung volumes and flow (vital capacity [VC], forced vital capacity [FVC], and forced expiratory volume in 1s [FEV1]), respiratory muscle strength (maximum inspiratory and expiratory pressure [MIP and MEP]), cough ability (peak expiratory flow [PEF] and peak cough flow [PCF]), vital signs (heart rate [HR] and respiratory rate [RR]), and arterial blood gases.
Secondary outcomes included adverse events, health-related quality of life, and functional performance.
Study selection and data extraction
Studies involving healthy adults (e.g., athletes) and those with respiratory conditions (≥18 years) were included. Participants aged <18 years were excluded due to anatomical and physiological differences between children and adults.19 Studies on kinesiology tape for non-respiratory muscles, subjective patient experiences, and outcome measures such as chest expansion, shape, and symmetry were also excluded.
Two reviewers independently screened the titles and abstracts, with full-text reviews performed by two others using Rayyan Software (https://www.rayyan.ai/). Discrepancies were resolved through discussion or by a fourth reviewer. Data extraction was performed by two reviewers using a self-collated form.
Risk of bias assessment
Two independent reviewers assessed risk of bias using the Cochrane Risk of Bias tool.20 Seven domains were evaluated: randomization, allocation concealment, selective reporting, blinding of participants or personnel, blinding of outcome assessment, incomplete outcome data, and other biases.
Non-randomized studies were evaluated with the Robins-I tool, including confounding, participant selection, intervention classification, missing data, outcome measurement, and selection of reported results.
GRADE assessment
The Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) tool was used to assess the certainty of evidence across studies.21 Five domains were assessed: risk of bias, indirectness, imprecision, inconsistency, and publication bias. Each domain was graded as not serious (no downgrading), serious (downgraded by one), or very serious (downgraded by two). For outcomes where only one study was included, inconsistency was not graded, as no comparison could be made.
Data analysis and synthesis
The meta-analysis was performed using SPSS v22 and Comprehensive Meta-Analysis version 4 (random effects). Means and standard deviations were used for FEV₁, PEF, MIP, and MEP in adults with respiratory conditions and MIP in healthy adults. The mean differences and variances were used for FVC, PEF, and FEV₁ in healthy adults. Heterogeneity was assessed with I² and publication bias for FEV₁ in respiratory conditions using Egger’s test. The significance level was set at α = 0.05. Outcomes exhibiting significant heterogeneity, precluding data pooling, were synthesized narratively and presented in a table.
Results
Study selection
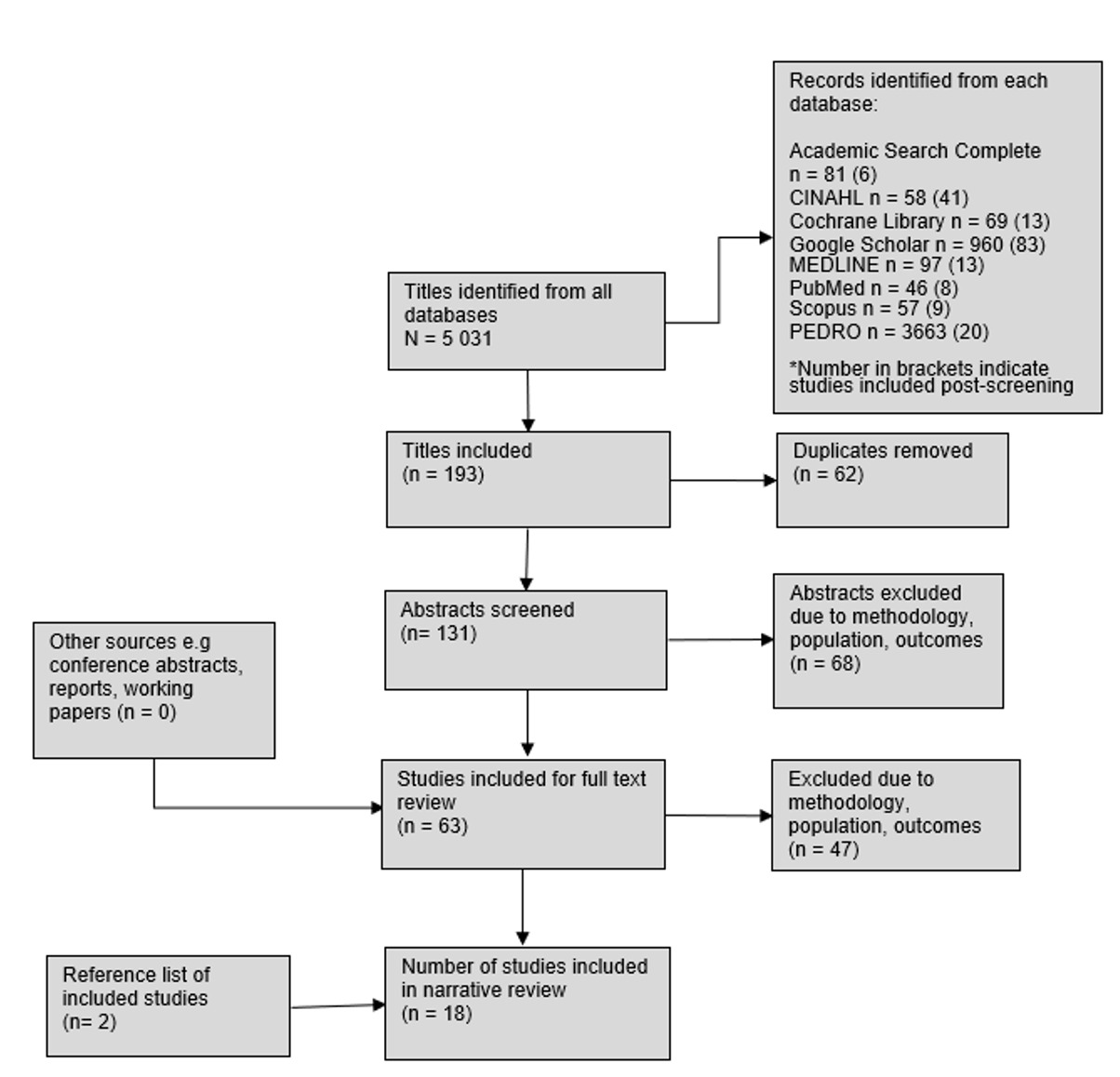
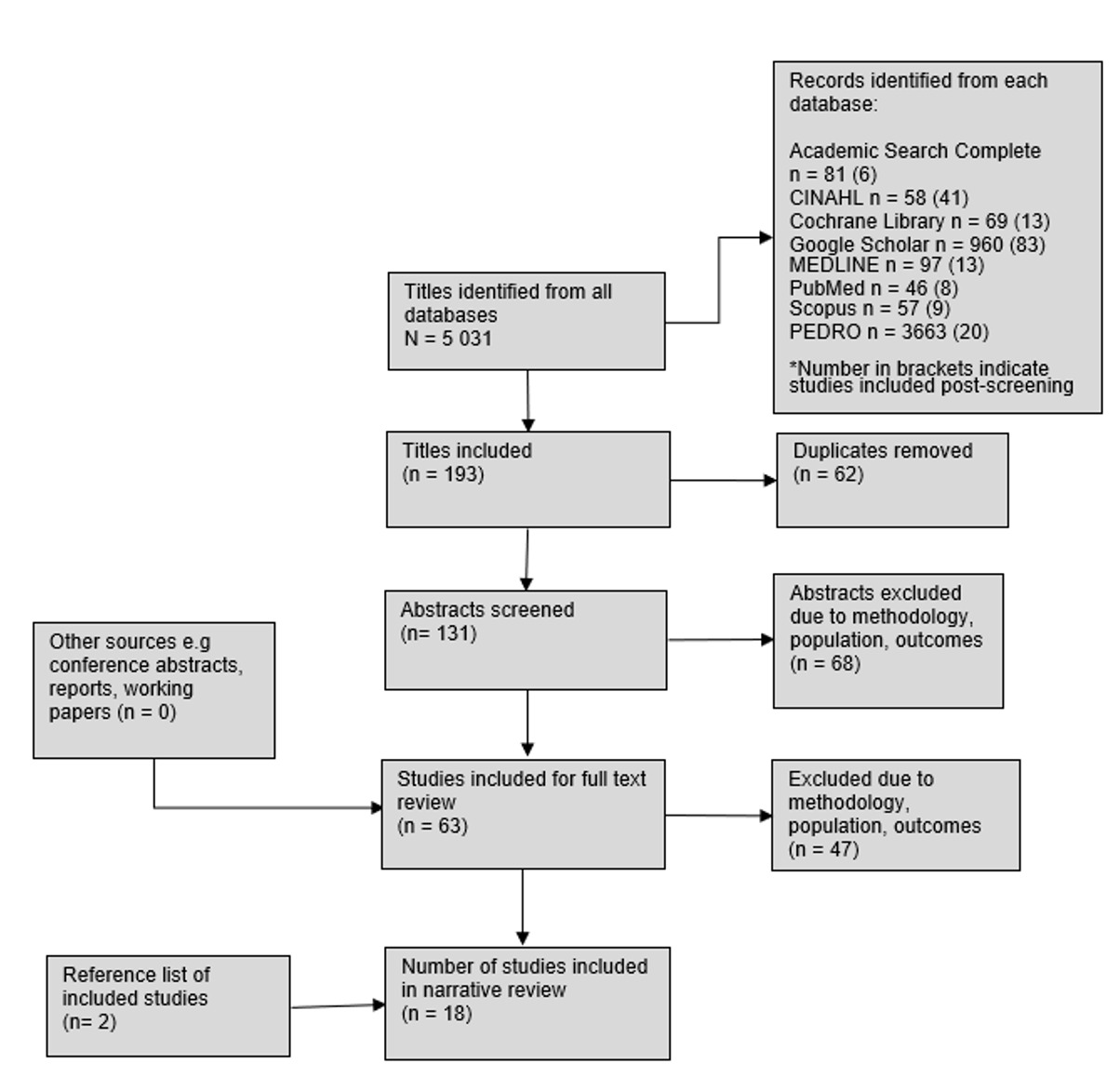
A total of 5,031 records were identified across eight databases. After initial screening, 193 titles were retained and 62 duplicates removed. Of the 131 abstracts assessed, 68 were excluded due to methodology, population, or outcome mismatch. Sixty-three full texts were reviewed, with 47 excluded for similar reasons. An additional two studies were identified from reference lists. In total, 18 studies were included in the final review (see Figure 1).
Participants
The review included 18 studies with 684 participants (316 healthy adults; 368 with respiratory conditions, mostly COPD) (see Appendix A), comprising 15 randomized controlled trials and three non-randomized studies. Sample sizes ranged from 10 to 90 participants, with more men than women, and four studies included only men. Healthy adults included sedentary individuals and those with varying activity levels, including runners and football players. Adults with respiratory conditions included those with severe COVID-19 pneumonia, mechanically ventilated patients, and those with various stages of COPD.
Risk of bias
Overall, 15 studies (83%) were judged to have a high risk of bias, as reported below.
Randomized controlled trials
Most studies (7/15) were a low risk of bias for absence of randomization, while one study was considered high risk and seven studies did not provide enough information to judge randomization. For allocation concealment, only three studies demonstrated a low risk of bias whereas 12 lacked sufficient detail for assessment.
For reporting bias, 10 studies were at low risk, while five were at high risk. Bias related to participant blinding was unclear in 12 studies, high in two, and low in one. Regarding blinding of outcome assessment, 11 studies lacked sufficient information, three were at low risk, and one was at high risk. With respect to incomplete outcome data, 11 studies had a low risk of bias, one had a high risk, and three were inconclusive due to insufficient information. Eight studies were highly suspected of other biases (e.g., performance or information bias), two were at low risk, and five did not provide adequate data.
Non-randomized controlled trials
Three non-randomized studies were assessed using ROBINS-I. One study had a moderate risk of bias, while two lacked sufficient information for assessment. For confounding, one study was judged moderate and two were inconclusive. One study had a moderate risk of bias for participant selection and intervention classification, while the remaining two provided insufficient information. None of the studies provided adequate data to assess bias from deviations in the intended interventions. All three had a low risk of bias due to missing data or selective reporting. All studies were rated as having a moderate risk of bias for the measurement of outcomes.
Respiratory function
Lung volumes and flows
In healthy adults, two studies demonstrated that kinesiology tape was superior to both sham tape and no tape in improving respiratory function (FEV1, FEV1/FVC).3,4 Additionally, kinesiology tape has been reported to reduce the duration of mechanical ventilation in adults hospitalized with unspecified respiratory conditions.1 In contrast, one study reported that kinesiology tape combined with IMT was not superior to IMT alone.22
For adults with respiratory conditions (mainly COPD), one study found significant improvements in FVC, FEV1, and FEV1/FVC, but only when kinesiology tape was combined with DBE.2 Other studies showed no superiority of kinesiology tape over unspecified, conventional physiotherapy,5,23 standard COPD treatment,24 incentive spirometry,9 DBE,6 or no tape25 in improving lung volumes and flows (see Table 1).
In two studies on healthy adults, kinesiology tape significantly improved PEF compared to sham tape,³ no tape, and tape without stretch.4 Kinesiology tape combined with IMT showed no significant improvement in PEF compared to IMT alone.22 Four studies on adults with respiratory conditions concluded that kinesiology tape is not superior to standard interventions in improving PEF.5,6,23,25
Respiratory muscle strength
Findings on respiratory muscle strength in healthy adults are contradictory. One study reported that kinesiology tape improved MIP and MEP,26 and another also found that kinesiology tape combined with IMT was superior to IMT alone in improving MIP.22 However, three studies found no significant improvement in MIP and MEP with kinesiology tape among healthy adults.4,27,28
For respiratory conditions, significant improvements in MIP and MEP were reported only during COPD exacerbation when comparing kinesiology tape to unspecified standard physiotherapy and medication.5,23 No significant improvement was found in stable patients with COPD when kinesiology tape was combined with DBE compared to DBE alone.6 See Table 2.
Vital signs and blood gases
Three studies on healthy adults found no change in HR, RR, or VO2 max when using kinesiology tape,4,10,29 while two studies omitted results for HR, blood pressure (BP)30 or SaO2.9 In adults with COPD exacerbation, kinesiology tape combined with standard physiotherapy and unspecified medication, improved SpO2 compared to standard intervention alone.5,23 However, in stable COPD, kinesiology tape had no significant effect on VO2 or SpO2.25 One study is however unpublished and not peer-reviewed; therefore its findings should be interpreted with caution.5,23
No studies have reported the effect of kinesiology tape on arterial blood gases, although one monitored them for safety without presenting values.30 See Table 3.
Secondary outcomes
Adverse events
Allergic reactions were reported in two sedentary adults after four days of taping,3 dermatitis in a runner after five days of use for four weeks,10 and itching in a COPD patient after one week of daily application.31
Hospitalization, morbidity and mortality rates
One study found no effect on intensive care unit (ICU) length of stay in patients with severe COVID-19 pneumonia when kinesiology tape was combined with standard ICU care and rehabilitation compared to standard interventions alone.1 While kinesiology tape did not affect mortality rates in these patients, it reduced the need and duration of mechanical ventilation.1
Health-related quality of life
No studies have assessed kinesiology tape and HRQoL in healthy adults. In moderate to severe COPD, tape significantly improved mental state on the Beck Depression Inventory (p < 0.001),24,32 possibly linked to improved respiratory function (FEV₁, FEV₁/FVC).
Functional performance
Two studies reported no significant effect of kinesiology tape with IMT on breathlessness, exertion, cycling, or the 6-minute walk test (6MWT).10,13 In contrast, taping improved aerobic capacity, shuttle run distance, and mechanical efficiency compared to sham3 and no tape.29
In respiratory conditions, three studies showed benefits when combined with physiotherapy, incentive spirometry,9 COPD treatment,24 or DBE,2 reducing dyspnea. However, two studies found no superiority over DBE⁶ or no tape,25 although minor gains in 6MWT were observed.6 Notably, taping with physiotherapy and incentive spirometry improved 6MWT9 and increased exercise duration by one minute.25
Quantitative synthesis
Effect of kinesiology tape on respiratory function in adults
Few outcome measures were pooled because of the heterogeneity of the included studies. Pooled results from two studies in healthy adults demonstrated no significant effect of kinesiology tape on FEV₁ (L/s) (Standard mean difference [SMD]: -0.078; 95% CI: -0.603 to 0.446; I² < 0.001), indicating negligible heterogeneity. Similarly, in adults with COPD, a pooled effect from five studies showed no significant improvement in FEV₁ scores (SMD = 0.42; 95% CI: -0.15 to 0.99; I² = 0.69; p = 0.15) despite substantial heterogeneity. Therefore, kinesiology tape had no significant effect on FEV1 in healthy adults or in adults with COPD.
Although individual effect sizes for FEV₁ varied, three studies including patients with COPD, favoured kinesiology tape (Cohen’s d = 0.24, 1.25, 0.40), while only one study favoured the control group (d = -0.14). One study that favoured the experimental group showed a significant large effect size (d = 1.25; p < 0.001) (see Appendix B), suggesting patients with respiratory conditions may benefit.
Grade assessment
The certainty of evidence for respiratory function was very low to low across all the cohorts (see Appendix C). No studies assessed the impact of kinesiology tape on respiratory muscle strength or arterial blood gas levels. Overall, evidence on the effect of kinesiology tape on respiratory function in adults is of very low certainty.
Discussion
This review evaluated the effect of kinesiology tape on respiratory function in healthy adults and those with respiratory conditions. Most studies included small samples with high risk of bias, resulting in low-certainty evidence. Considerable variation in taping techniques, targeted muscles, and participant characteristics limited the meta-analysis. No significant effect of kinesiology tape on outcomes such as FVC, FEV₁, PEF, MIP, or MEP was found. However, several individual studies suggested potential benefits, particularly in patients with respiratory conditions.
Lung volumes and flows
Findings on healthy adults were inconsistent. One study reported no significant improvement of lung volumes and flows after four weeks of diaphragmatic kinesiology tape combined with IMT,22 while two studies reported significant improvement after kinesiology tape application.3,4 These differences may reflect variations in taping duration and physical activity levels, which influence respiratory muscle adaptation.33 Improved PEF was observed in physically active adults with abdominal taping, likely due to greater expiratory muscle engagement.4,34 Taping might therefore be more effective when paired with activity. This aligns with studies demonstrating that abdominal muscle activation affects forceful exhalation, particularly in individuals with compromised respiratory function.35
In respiratory conditions, the pooled results showed no significant improvement for FEV1, although one study combining kinesiology tape with DBE in patients with COPD reported a large effect favouring kinesiology tape.2 Therefore, kinesiology tape may be more effective in adults with respiratory conditions than in healthy adults. Adults with respiratory conditions such as COPD present with various limitations, including compromised respiratory muscle strength,36 severe airflow obstruction, and hyperinflation.37 Although direct comparisons are lacking, kinesiology tape appears to show measurable effects in compromised respiratory muscles,2,6,23,25 while studies in healthy adults report minimal effects or inconsistency.3,4,26–28 This suggests that kinesiology tape may be clinically more effective for muscles with compromised respiratory function.
Kinesiology tape combined with DBE for six weeks showed no superiority over DBE alone in improving respiratory function,6 suggesting kinesiology tape alone may not enhance function. The effect of kinesiology tape may vary with COPD duration and stage, as improvement was noted in adults diagnosed for >5 years,2 unlike studies with unknown disease duration.6 Longer disease duration is associated with increased thoracic stiffness and reduced lung compliance,38 conditions that kinesiology tape may help mitigate by improving posture and rib cage mobility. The effect of kinesiology tape may be too small to detect a significant difference between groups. Studies with single kinesiology tape application reported no significant improvements,5,9,23 indicating repetitive, longer use may be required.
Respiratory muscle strength
Conflicting evidence exists on kinesiology tape improving respiratory muscle strength (MIP and MEP), possibly because the diaphragm’s unique shape may complicate effective taping.6 Three studies in healthy adults suggest no significant effect, which may be due to their already optimal respiratory muscle function, leaving little room for improvement.4,27,28 One study reported significant muscle strength improvement with frequent kinesiology taping,26 whereas another study observed no effect with a single-day application,28 Therefore, potential benefit might be greater in adults with respiratory muscle weakness and when taping is applied regularly as compared to a once-off intervention. These mixed findings underscore the need for further research to confirm the effectiveness of kinesiology tape and its optimal application duration for respiratory muscle strength.
Two studies on COPD exacerbation found no significant improvement in muscle strength between groups, with within-group gains likely due to symptom recovery rather than kinesiology taping.5,23 Respiratory muscle strength typically improves markedly at one month post-exacerbation without kinesiology taping.39 Studies in patients with stable COPD showed no significant muscle strength improvement with kinesiology tape application.2,6,9,24,25 Kinesiology taping significantly improved SpO2 only during COPD exacerbation,5,23 but showed no improvement in stable patients,9,25 indicating that clinical value may be limited to short-term supportive intervention during acute episodes rather than routine use in stable COPD.
Secondary outcomes
Adverse events were minor and mostly limited to skin irritation,3,10 suggesting that kinesiology tape is generally safe for clinical use. In COVID-19 patients, kinesiology tape reduced ventilation needs but did not affect ICU stay or mortality.1 Because quality of life is often markedly impaired in COPD, especially among women,40 there is a need for studies with greater female representation to guide sex-specific clinical decision-making.
In COPD, taping respiratory muscles improved physical activity and exercise duration,25 and with incentive spirometry and physiotherapy, enhanced 6MWT in mild to moderate disease.9 In moderate to severe COPD, taping with DBE yielded only minor improvements,6 likely from reduced dyspnea, fatigue, or a learning effect.
Thoracic application may support expiration by enhancing elastic recoil, reducing residual volume and hyperinflation.6,29,41 However, Tomruk et al.6 reported benefits were short- to medium-term, with no lasting effect on dyspnea. Therefore, clinicians should view kinesiology taping as a temporary supportive intervention rather than a long-term solution.
Limitations
Four studies were published in foreign languages, where translation software may have reduced accuracy, and one unpublished dissertation lacked peer-review rigour. Small subgroup sizes also limited meta-analyses.
Most studies were rated as having low to very low certainty, which reduced their clinical applicability. The absence of critical appraisal and the inability to perform statistical comparisons further limited the reliability and assessment of between-group differences.
Implications and recommendations
The review summarizes the current evidence on the use of kinesiology tape for respiratory function in healthy adults and patients with respiratory conditions. Overall, no significant effects were found, and support for its use, even as an adjunct, remains limited.
Future trials should be more rigorous, as outcomes may vary depending on the tape type, application method, and potential bias. High-quality studies focusing on patients with conditions such as COPD and exacerbations are needed, incorporating measures like chest shape, posture, and expansion to better inform respiratory assessment.
Conclusion
This systematic review and meta-analysis found no consistent evidence that kinesiology tape improves respiratory outcomes such as lung volumes, flows, or respiratory muscle strength in adults. Nonetheless, the effect sizes and findings of individual studies suggest that certain patients may derive benefits. Larger, methodologically robust trials with standardized taping protocols are needed before kinesiology tape can be recommended as part of routine respiratory care.
Acknowledgements
The authors extend their gratitude to the information specialists Mrs. Estelle Grobler, Mrs. Glenda Makate and Mrs. Monica van Schalkwyk for their assistance with the search strategies. Special thanks to Dr. Nweke for statistical assistance and to Anne-Joline Stonlake for language editing.
Competing interest
The authors declare that they have no competing interest.
Authors contributions
Charlene du Plessis conceptualized and collated the systematic review, with input from all co-authors. Charlene du Plessis led data collection. Study screening was undertaken by Charlene du Plessis along with Prof. Anri Human and Dr. Rubine Brandon. Data extraction and analysis of the included studies were conducted collaboratively by Charlene du Plessis and Prof. Anri Human. Prof. Anri Human, along with Charlene du Plessis, drafted the first version of the manuscript, while editing and proofreading were performed by all authors.
Funding information
This research did not receive any funding from a grant, institution, or any other public, commercial, or nonprofit sectors.
Data availability
Data can be made available upon request from the corresponding author.
Disclaimer
The views and opinions in this study are from the authors’ own, and not from the official position of the institution or funder.
AI Statement
During the preparation of this work the author(s) used OpenAI’s ChatGPT in order to shorten sections to adhere to the word count. After using this tool, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication