Introduction
Home mechanical ventilation (HMV) provides positive airway pressure support for patients with chronic diseases leading to progressive respiratory failure, including neuromuscular disease, chronic obstructive pulmonary disease (COPD) and/or failure to be weaned from mechanical ventilation after the onset of acute respiratory failure.1 HMV can be provided non-invasively via a mask or mouthpiece or invasively via a tracheostomy tube. The prevalence of HMV has increased over the last few decades worldwide.1–3 There are an estimated 12.9/100,000 patients using HMV in Canada, and the population continues to grow.1 These individuals represent one of the most vulnerable patient groups in the country with significant healthcare utilization.3,4
Philips Respironics is a division of the global Philips Healthcare company and focuses on sleep and respiratory care.5 In June 2021, Phillips Respironics issued a global voluntary field safety notice (countries outside the USA) and voluntary recall (USA only) for their positive airway pressure and mechanical ventilator devices, including the Trilogy 200 devices.6 The recall was issued to address potential health risks related to the breakdown of the polyester-based polyurethane (PE-PUR) sound abatement foam (which reduces noise and vibration) in the affected devices.6 This exacerbated ventilator equipment scarcity from the COVID-19 pandemic and caused a significant issue for ventilator-assisted individuals and healthcare teams worldwide.7 In Ontario, Canada, HMV equipment is provided through the Ventilator Equipment Pool (VEP), a provincially funded program where patients must meet specified criteria to be eligible. This global recall had a significant impact in Ontario, as the Trilogy 200 was the most frequently prescribed device for invasively ventilated and certain complex non-invasively ventilated patients. Patients and families were notified of the next appropriate steps through guidance from Phillips Respironics, VEP and their HMV clinical teams. The VEP introduced the ResMed Astral 150 and Phillips Respironics EVO devices as replacement options for the Trilogy 200 ventilator in the Fall of 2021; however, the Phillips Respironics EVO device later had recall issues related to pressure delivery, leaving only a single device for use.8
Currently, there is no standardization for HMV devices, and each company has its own nomenclature, variety in circuit setups, performance variability and proprietary equipment.9–12 Multiple studies have shown that home mechanical ventilators demonstrate patient ventilator asynchrony and variable tidal volume delivery at higher pressure settings, decreased inspiratory muscle effort and variable leak issues affecting gas exchange and patient comfort.10–12 This poses unique challenges when switching fragile individuals with medical complexities from one ventilator device to another, requiring careful planning and monitoring. This is critical in the pediatric population, as they require more personalized care given their physiology and the need for ongoing evaluation and adjustments as they grow and develop. The aim of this narrative review is to outline the key clinical considerations for transitioning between home mechanical ventilators, based on an appraisal of existing literature over the last 20 years, and to support the creation of a key consideration checklist.
Methods
A narrative review was conducted to evaluate and describe the current knowledge and evidence available for home mechanical ventilator transitions in ventilator assisted individuals (VAI). This approach is flexible, provides relevant synthesis of diverse study designs and literature, promotes learning about a topic and is useful in highlighting areas for further research13,14 Although there are no standard reporting guidelines for narrative reviews, we completed our review systematically using Covidence.13,14
The search strategy was developed in collaboration with JC a professional medical librarian and executed in the following bibliographic databases on November 5, 2024: Ovid MEDLINE(R) ALL and EBSCOhost CINAHL Plus). MEDLINE ALL was chosen, as it represents a comprehensive body of biomedical literature. CINAHL Plus was chosen because it contains literature pertinent to the professional disciplines and the delivery of care involved in transitioning patients on mechanical ventilation to home settings. Online records were uploaded to Covidence, which then removed duplicate records. NC completed the title and abstract review of the collected studies. If the article was considered potentially relevant, it was accepted into the next phase for determination of eligibility. Initially, there was no restriction on the publication year; however, to ensure focus on modern home mechanical ventilators utilizing turbine flow technology, studies from 2005 to 2025 were prioritized.15 Modern turbine home ventilators use electrically powered blowers to provide air flow and have been shown to be as efficient in trigger response and pressurization as ICU ventilators using high pressurized gas systems for air flow.15
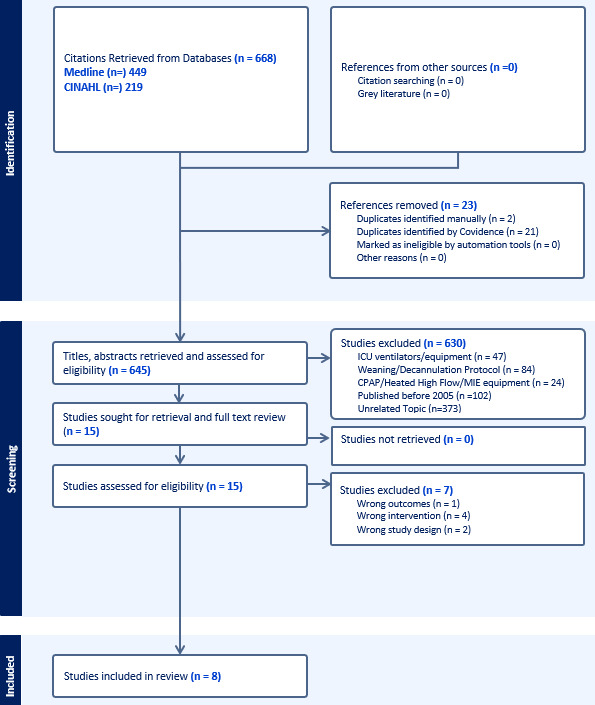
Full-text articles were then screened independently by two reviewers, NC and CB, for inclusion. Disagreements at this stage were reviewed by SM, a third experienced reviewer, for consensus. The two reviewers independently assessed the quality of the studies for inclusion into the extraction phase using the JBI Critical Appraisal Checklist for case series, cohort studies, quasi-experimental studies and textual evidence.16–19 Fifteen articles were evaluated in the full text review, eight articles were agreed to be eligible and included in the extraction phase following critical appraisal. One article on pediatric transition from an ICU ventilator to a home mechanical ventilator was included among the extracted articles following reviewer consensus, despite the exclusion criteria for ICU ventilators and equipment. The article explored key considerations such as a standardized protocol, readiness assessment and interdisciplinary teamwork which are relevant and adaptable for home-to-home mechanical ventilator transitions.
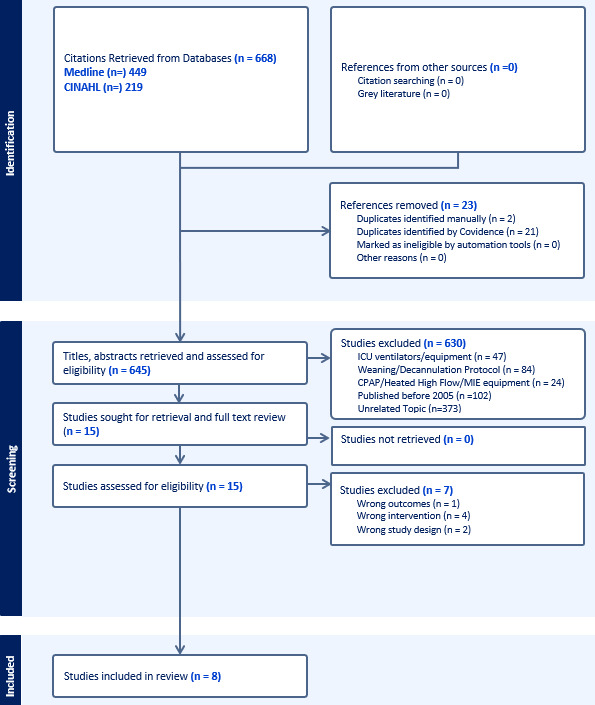
The two reviewers independently extracted information from each study using a modified Covidence data extraction template that follows the PICOT structure (patient, intervention, comparison, outcome, and time) and enabled consistent data collection across all included studies. Then the two reviewers compared their extracted data to discuss discrepancies and finalize the data for analysis. The data was extracted as described in the articles, then summarized and grouped into themes. See Figure 1 for the PRISMA flow diagram and see supplementary information for the detailed search strategy description.
Results
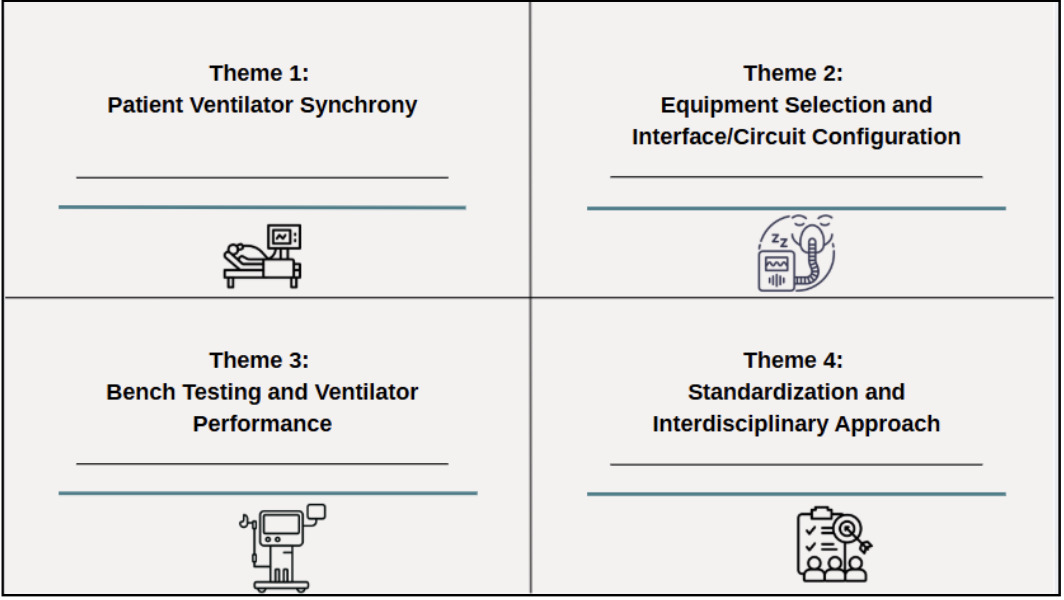
The narrative review identified four themes as key considerations for home mechanical ventilator transitions: Patient Ventilator Synchrony, Equipment Selection and Interface and Circuit Configurations, Bench Testing and Ventilator Performance, and Standardized and Interdisciplinary Approach (see Figure 2).

Patient Ventilator Synchrony
Patient ventilator synchrony plays a key role in a successful home ventilator transition. Appropriate and highly sensitive trigger and cycle mechanisms, patient inspiratory effort, ventilator pressurization capacity, management of unintentional leak, and airway mechanics are all essential considerations.15,20–26 Poor and/or ineffective trigger and cycle sensitivity from poor ventilator choices or incorrect settings will result in patient ventilator asynchrony leading to transition failure, sleep disruptions, reduced therapy effectiveness, poor compliance, increased patient discomfort, fatigue, and potential worsening of the underlying respiratory condition.20–22,24,26 Close monitoring with respiratory assessments including breathing rate, accessory muscle use, oxygen requirements, carbon dioxide levels, auscultatory changes and secretion management, with real-time adjustments to optimize synchrony can improve post transition outcomes.26 Utilizing telemedicine, ventilator data downloads and regular follow ups are highly recommended for re-evaluation, ensuring ventilation effectiveness, optimized settings and prompt management of patient ventilator synchrony issues.15,21–24,26 Interface and circuit configurations also influence patient ventilator synchrony.15,22 Hence, ensuring effective patient ventilator synchrony and continued monitoring is essential for successful home mechanical ventilator transitions.
Equipment selection and interface and circuit considerations
For optimal respiratory support, it is critical to choose a ventilator that best suits the patients’ needs by considering their primary diagnosis, ventilation type (non-invasive vs invasive), patient weight, ventilation dependency (hours used/day), alarm configurations, battery support requirements and portability.15,20–22,24,25 There are no standardized, international regulations for home mechanical ventilator devices and they can be prescribed based on patient usage, weight criteria, or, as in Canada, based on the risk associated with their usage.20,27 In France, home mechanical ventilators are classified into three regulatory categories based on patient weight and device complexity.20 Level I devices include CPAP for patients > 30 kg and BiPAP for those >13–18 kg, while Level II devices are for patients >10–13 kg.20 Level III devices are considered life-support and utilized for vulnerable patients, supporting > 2.5–5 kg, depending on manufacturer guidelines.20 Levels I and II devises are simple and compact with integrated humidifiers.20 Whereas Level III devices are bulkier, more advanced with external humidifiers, sophisticated alarm systems and internal battery backup20 In Canada, CPAP and BiPAP devices are categorized as Class II while ventilator devices are Class III depending on the level of invasive support provided.27,28 Home ventilator circuits vary in design and performance, each with specific advantages and limitations.22 See Supplementary Information (Table 3) for a summary table of currently available HMV devices in Canada.
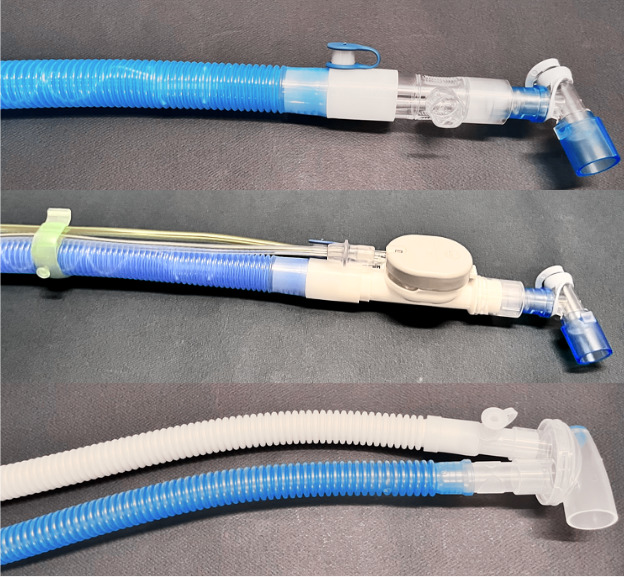
There are three circuit setup options available for home mechanical ventilators (see Figure 3), and each type influences monitoring, ventilator performance, patient comfort, respiratory workload, and therapy effectiveness.15,20,21,25,27 Circuit compatibility must be considered when transitioning between ventilators as some circuit setups may not be available on the new ventilator.24 Matching the circuit configurations and settings as much as possible between ventilator devices is essential for maintaining ventilatory support and reducing adverse effects during transitions.23,26 The single limb circuit setups, which include vented/passive leak circuits, and the active exhalation circuit, are recommended for intermittent or nocturnal ventilation usage.24 The vented/passive leak circuit has a continuous leak with a simple, lightweight setup and is the most commonly used circuit for HMV.15,20–22,24 However, it provides indirect estimated expiratory ventilation data (i.e., tidal volume, minute ventilation) and is sensitive to asymmetric leaks that may disrupt ventilator performance.22 The active exhalation circuit has a valve attached at the distal end of the circuit with a controlled leak by the ventilator during expiration phase and provides estimated inspiratory ventilation data.15,20–22,24 It can effectively prevent carbon dioxide rebreathing but can be complex to set up, and clinicians may struggle with accurate volume and leak estimations.22 The double/dual circuit setup has a separate inspiratory and expiratory tubing connected by a Y-piece with no need for anti-rebreathing valves.15,20–22,24 This setup provides the most accurate inspiratory and expiratory ventilation data, however, the setup is bulky, sensitive to unintentional leaks and can underestimate tidal volume in pressure modes due to compressible volume loss.15,20–22,24
__single_limb_circuit_with_passive_leak.png)
It is very important to minimize circuit dead space to improve patient comfort, synchronization and volume delivery.26 Clinicians should have a clear understanding of the air flow dynamics through each type of ventilator circuit, as this is crucial for accurately interpreting ventilation data and making appropriate settings adjustments.22
For non-invasive HMV, the correct type of mask interface is critical for effective ventilation therapy, especially in pediatric patients, as poor fit leads to discomfort and reduced compliance.20–22 Careful mask fitting and regular monitoring are essential to minimize complications related to long-term interface use, including midface hypoplasia, maxillary retrusion, eye irritation and oronasal dryness.20,21 The presence of an internal battery with an external battery attachment is essential to ensure uninterrupted ventilatory support during travel, equipment malfunction, or power outages.15,21 Additionally, with the growing use of telemedicine and digital care models, remote monitoring and downloadable ventilator data are essential considerations for continuity of care and timely clinical management.21 The healthcare team’s preference and knowledge of the ventilator device, comfort with usage/setup and ability to troubleshoot can promote improved patient and caregiver comfort and clinical outcomes.24–26 Patient-centered care through appropriate selection of the ventilator device, circuit configuration and interface combined with healthcare provider expertise will further support a smooth home mechanical ventilator transition.
Bench testing and ventilator performance
The variability and differences in ventilator algorithm, nomenclature, mode/settings options and performance across manufacturers can further complicate ventilator transitions.23,25,26 Bench testing, using either artificial lungs or simulators, is very important in evaluating ventilator performance as emphasized by Martinez et al.24 who assessed the performance of 8 home ventilators under 18 different conditions combining 3 types of patient mechanics and 2 inspiratory effort levels. They evaluated volume delivery, trigger response, pressurization capacity and quantity/quality of the asynchronies developed and demonstrated the significant response variability of these outcomes across all the devices under identical settings.25 This work highlighted that effective synchronization is dependent on sensitive trigger response and pressurization capacity which are both essential for reducing patient respiratory effort, especially considering that leaks are an unavoidable aspect of HMV.
Overall, the ventilator devices varied in tidal volume delivery and lacked accuracy in the tested conditions.25 In volume control–continuous mandatory ventilation (VC-CMV), most ventilators demonstrated a notable decrease in tidal volume delivery when inspiratory effort was low. Trigger response also varied with longer delays compared to previous studies, especially under low inspiratory effort.25 This affected pressurization capacity which ranged from 0 to 77% with an asynchrony index of 2 to 76% across the devices.24 In this study, the ResMed Astral 150 ventilator showed limitations in synchronization and volume delivery in the obstructive and restrictive patient mechanics during pressure support of 20 cmH2O (PSV20) and delivered significantly lower tidal volume of 215 mL (expected was 1000 mL) in the obstructive patient setting.25
In contrast, the Phillips Respironics Trilogy Evo ventilator demonstrated accurate and consistent performance across most conditions. It maintained appropriate tidal volume delivery in low effort scenarios as well as with obstructive and restrictive lung mechanics.25 The Trilogy Evo device also maintained synchrony across various ventilatory modes and mechanics, showing minimal therapy disruption.25 Bench studies have also demonstrated the effects of asymmetric and intermittent leaks on tidal volume delivery and pressure data in single limb passive circuits, as well as, inability to compensate for leaks or weak inspiratory effort.20,22 Khirani et al.,20 highlighted that detailed pressure and flow wave forms are valuable for detecting asynchrony issues identified during bench testing.20 Bench testing studies have demonstrated the variability amongst home mechanical ventilators and understanding the difference between the previous and new home device is critical for patient comfort and transition success.
Standardization and interdisciplinary approach
Two articles demonstrated protocolized approaches to home mechanical ventilator transitions, with Willis et al.26 focusing on transition from an ICU ventilator to a home ventilator, while Brandt et al.23 discussed their transition approach from the Philips Respironics Trilogy 200 device to an alternative non-recalled device. Willis et al.26 hypothesized that utilizing a standardized protocol for transitioning to a home ventilator would lower the number of failed attempts for children under three years of age requiring long-term ventilation in the Arkansas Children’s neonatal and pediatric ICU. Although this protocol describes transition from an ICU device to a home device, it was included in the review for exploring transferable concepts that can be applied to home mechanical ventilator transitions. They retrospectively collected data with pre-protocol patients (n = 27) recruited from 2011-2014, and post-protocol patients (n = 28) recruited from 2015-2018.26 No significant demographic or clinical differences were found between the two groups in terms of age, gender, diagnosis distribution and disease severity.26 Key features of the protocol included standardized criteria for the transition, a readiness assessment, ventilator mode and settings recommendations, heightened observation and monitoring, consistent detailed documentation during the transition attempt and transition failure criteria with multi-disciplinary discussion to evaluate the cause for failure.26 The attending pulmonologist would ensure adherence to the protocol, which began with the patient readiness assessment; a holistic respiratory and non-respiratory stability evaluation.26 This included confirmation of stable ventilator settings, a normal chest radiograph, no sedation withdrawal symptoms, and good growth and nutrition.26 Utilizing the same home ventilator for transitions, PC-SIMV mode and matching to ICU ventilator settings supported consistency and standardization.26 Heightened monitoring of the patient’s baseline work of breathing (WOB), ventilation data with detailed documentation were completed 24 hours prior to the transition and 48–72 hours post transition.26 Specific failure criteria, including increased WOB, elevated oxygen requirements or elevated carbon dioxide (PCO2), and ventilator-patient asynchrony, were highlighted to support timely assessment and discontinuation of transition.26 The failure criteria established general assessment considerations and were adjusted based on each patient’s baseline values, demonstrating that a standardized protocol can still be patient-centred.26 A successful transition was defined as maintaining stability on the home ventilator for at least 14 days without signs of intolerance.26 Implementation of the structured protocol (see supplementary information) led to significant decreases in the total number of transition attempts (3.3 ± 2.7 to 1.6 ± 1.1, p = .005) and the number of failed transition attempts (2.3 ± 2.7 to 0.6 ± 1.1, p = .005) for their pediatric patients.26 They also noted a significant reduction in the time to successful transition (67 ± 90.7 days to 17 ± 28.6 days, p = .01), decreased length of stay in the ICU (13 ± 6.4 months to 9 ± 4.5 months, p = .05) and significant reduction in mean length of time for initial attempt with a home ventilator to successful transition (67 +/- 90.7 d to 17 +/- 28.6 d, p = .01).25 This study demonstrated that the use of a standardized ventilator transition protocol decreased failed attempts, shortened the length of time to a successful transition, and improved patient outcomes.26
Brandt et al.23 described the clinical course of their invasively ventilated patients with Trilogy devices undergoing an inpatient transition to alternative home ventilators through implementation of an institutional protocol. The protocol was developed with consensus from their pediatric pulmonology division and prioritized patient-centered care and shared decision-making with patient and family caregivers.23 They chose the inpatient environment for close monitoring, parental training and safe real-time adjustments.23 They retrospectively reviewed the transitions that occurred from July to September 2021 in the technology-dependent intensive care unit (TICU) of Children’s Healthcare of Atlanta-Egleston.23 During this time, they transitioned 19 patients to the Breas Vivo 65 (n = 13) and ResMed Astral 150 (n = 6) based on the ventilator availability of the patient’s dural medical equipment (DME) company.22 There were fourteen male patients (74%) in the cohort, eight patients (42%) received nocturnal invasive ventilation and median age was 5.9 years (IQR: 9.5 years).23 They prioritized patients who were already hospitalized, scheduled for elective post-op admission or symptomatic per Philips Respironics recall criteria, with eleven patients (58%) meeting this criteria.23
The process started with patient/family discussion and planning for transition with equipment arrangement from the DME company.23 During the admission, the patient was monitored on their Trilogy home settings for at least 30 minutes with assessment of oxygen saturation (SpO2), capillary blood gas (CBG), and/or end-tidal carbon dioxide (ETCO2.23 If there were no concerns, the patient was transitioned to the alternative device on matching settings with close continuous monitoring of SpO22, ETCO2 and work of breathing with a CBG 1- 4 hours post transition.23 Settings were adjusted accordingly, and patients were monitored overnight.23 Patients were discharged home following caregiver education with outpatient clinic follow-up the next day and one week post-transition.23 The median hospital stay was 2 days (IQR: 6 days), with shorter admission observed in cases involving only a ventilator change.23 There were no reported issues with insurance coverage for the new ventilators, and overall, no major complications were reported within one week post-transition.23 Two patients required ventilator setting adjustments post transition during the admission: one for hypercapnia and one with a planned weaning.23 One patient required outpatient alarm adjustments.23 A systematic and collaborative approach using a protocol-optimized home mechanical ventilator transitions.23
Interdisciplinary collaboration and patient-centered care are essential for successful home mechanical ventilator transitions, as they ensure appropriate ventilator selection, safe configuration and settings, timely family education, and shared decision-making amongst interest holders, including respirologists, respiratory therapists, nurse practitioners, DME providers, home care nursing, patients and family caregivers.15,20–26
Pediatric Considerations of the Four Themes
Pediatric patients have several unique physiological factors that put them at higher risk of respiratory failure and decompensation that may affect their tolerance of a new home mechanical ventilator and overall success of the transition.29 Infants have immature respiratory control and present with periodic breathing and apneas (less than 20 seconds is considered normal) that improve with maturity and growth.29 They also have smaller upper and lower airways, which are more susceptible to collapse due to lower muscle tone, smaller airway diameter and increased compliance.29 Additionally, pediatric lungs have fewer alveoli and reduced gas exchange surface area.29 When combined with their higher metabolic rate and increased oxygen consumption, infants and young children have lower respiratory reserve and faster decompensation when unwell or inadequately supported.29
These factors emphasize the importance of appropriate trigger sensitivity especially for pediatric VAI, as their respiratory needs are more dynamic due to their general growth, activity level, and impact of the disease on their respiratory muscles and drive to breathe; making this population more sensitive to ventilator bias flow and device dynamics.20–23,26,30 There are no dedicated pediatric-specific home ventilators available on the market. However, recent improvements have led to home ventilators providing lower tidal volumes (as low as 35 mL), improved trigger sensitivity to lower flow demands, and approved for weight limits down to 2.5 kg.15,20,21
Choosing the correct ventilator device, circuit configuration, and appropriately sized interface for pediatric VAI will reduce the risk of decompensation due to inadequate ventilation and help maintain compliance and patient tolerance to therapy on the transitioned device. Some home ventilator devices include an option to add a proximal flow sensor for improved inspiratory flow detection in the presence of leaks and for pediatric ventilator-assisted individuals due to their lower inspiratory flow rates.15 Modern home ventilators can compensate for circuit dead space and compressible volume loss through circuit pre-use checks, which is an important consideration for pediatric patients requiring smaller tidal volume delivery.15 For example, we may consider a dual limb circuit setup with a cuffed tracheostomy tube for invasive ventilation of a severe bronchopulmonary dysplasia infant for optimal trigger sensitivity, accurate pressure delivery, consistent volume support and controlled CO2 clearance. Children who are dependent on higher ventilator pressures for lung expansion and adequate gas exchange will not have to work as hard to breathe on a dual limb circuit compared to a continuous or intermittent leak that is present with the other two single limb setups.15,20,29
When benching testing a home mechanical ventilator, it is important to include pediatric-focused testing conditions, such as assessing smaller tidal volume delivery, alarm sensitivity and response with pediatric-sized interfaces and pressurization response to high airway resistance and lower inspiratory flow demand.29,30 One study demonstrated the absence of low inspiratory pressure alarm notification for simulated tracheostomy decannulation under 5.0 mm ID and there have been reports of various alarms not being triggered during accidental decannulations for smaller tracheostomy tube sizes due to the lack of pressure drop or occlusion by patient and other materials.30
Finally, a standardized and interdisciplinary approach that can be catered to the patient’s specific context and needs is important for pediatric VAI as it will support thorough transition planning, promote consistent communication with patients and families, ensure clear monitoring criteria and follow-up expectations to optimize safety and effectiveness during the home mechanical ventilator transition.26,30
Discussion
The global Phillips Respironics recall highlighted the critical need of resource management and diverse inventory for home mechanical ventilator devices. This narrative review has highlighted four themes of key considerations for ventilator transitions: Patient Ventilator Synchrony, Equipment Selection and Interface and Circuit Configurations, Bench Testing and Ventilator Performance, and Standardized and Interdisciplinary Approach (Figure 2).
Home mechanical ventilator transitions are complex and require careful planning with an interdisciplinary approach to reduce adverse effects and improve patient outcomes, caregiver burden, and healthcare utilization.15,20–26 This is a result of the variability in home mechanical ventilator device configurations, and performance demonstrated through bench testing studies across modes and patient lung mechanics.15,20–26 While these differences may have minimal impact on older children and adults, there may be clinically significant effects on infants and younger children due to their fragility, lower oxygen reserves and immature respiratory control, which can be more pronounced in children with neuromuscular weakness.15,20,21,25,26,30 Although the ResMed Astral 150 device was previously shown to perform well in the presence of leaks and lower inspiratory effort, it was not reproducible by Martinez et al.,25 emphasizing performance variability under different scenarios, including the home environment.25 It is paramount that healthcare providers have a thorough understanding of the ventilator devices they recommend for their patients, including circuit configuration options, air flow dynamics, secondary settings (trigger, cycle, inspiratory time and rise), and effects on patient ventilator synchrony.24–26
Comprehensive bench testing of all ventilator features and/or review of existing bench testing literature for the chosen ventilator is highly recommended to optimize patient care, guide proper setting adjustments, and ensure patients are transitioned to devices that align with their individual needs. A transition readiness assessment is also crucial to ensure patients are at their clinical baseline and appropriately prepared from a respiratory and non-respiratory lens.26 Family caregiver readiness for the ventilator transition should also be included in the assessment, which was not specifically highlighted in the reviewed articles.29,31 There is a significant care burden (physical, emotional and financial) on family caregivers of ventilator-assisted individuals, particularly for invasively ventilated children who require 24 hours/day of care with an awake, alert caregiver.29,32 Ensuring that family caregivers have the physical, emotional, and financial capacity to collaboratively participate in planning and execution is critical for successful and sustainable ventilator transitions. Additionally, establishing clear criteria for transition failure is important to promptly identify and address any signs of intolerance or clinical instability.26
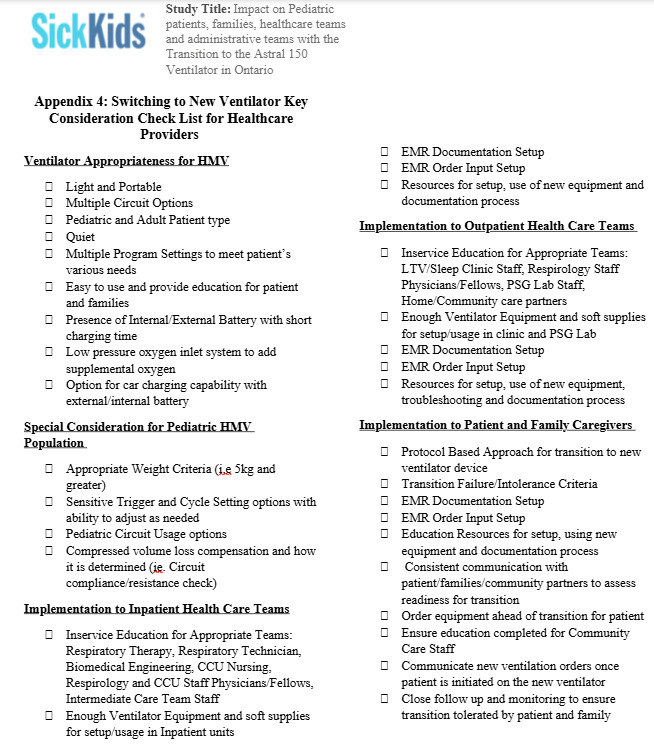
A basic home mechanical ventilator transition checklist was created from the knowledge and insight gained from this narrative review (see Figure 4). This checklist will be further refined through a qualitative study with key interest holders, including patients, family caregivers, and HMV experienced healthcare providers.

Brandt et al.23 highlighted key challenges to their in-hospital ventilator transition protocol, including limited supply of non-recalled home ventilator devices from the DME company and limited ICU bed availability. Establishing and maintaining clear communication pathways among all ventilator transition interest holders can foster interdisciplinary collaboration, enhance efficiency and improve care coordination. Further randomized control trials and implementation of ventilator transition guidelines, including the outpatient context and research on long-term patient outcomes related to home mechanical ventilator device transitions, are needed to strengthen clinical decision-making, support standardized practices, and improve patient and caregiver experiences.
Limitations
This narrative review has several notable limitations. The initial title and abstract screening was conducted by a single reviewer, which may introduce selection bias. However, all subsequent stages of the review involved two independent reviewers to enhance reliability. Of the eight articles included, six were also narrative reviews. While these provide valuable and broad perspectives on the topic, they may lack the methodological rigour of systematic reviews or empirical studies. However, this is the reality of this understudied topic. Additionally, we acknowledge that our literature search could have been further improved by conducting an independent, parallel search for related articles to enhance the comprehensiveness of the identified themes and reduce potential bias. Despite these limitations, the articles reviewed offered rich, consistent, and highly relevant insights into key considerations for ventilator transition and the need for standardized protocol implementation.
Conclusion
The rising prevalence of home mechanical ventilation, combined with the need for diverse ventilator devices to support a heterogeneous patient population and rapid technological advances, creates significant challenges for HMV device transitions. Evidence-based clinical guidelines and standardized protocols can support healthcare teams in improving patients’ and family caregivers’ experiences, while also helping to reduce stress and uncertainty during the transition process. Standardized approaches to ventilator transitions can facilitate consistent decision-making, promote effective communication among interdisciplinary teams, ensure continuity of care, and minimize the risk of clinical errors or adverse patient complications.
Contributions
All authors contributed to the conception or design of the work, the acquisition, analysis, or interpretation of the data. All authors were involved in drafting and commenting on the paper and have approved the final version.
Declaration of conflicting interests
All authors have completed the ICMJE uniform disclosure form and declare no conflict of interest.
Ethics approval
Not required for this article type.
AI Statement
During the revision of the manuscript for CJRT, Copilot was used to proofread English (word choice, grammar, fluency) and improve readability. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Funding
This narrative review is part of a mixed-methods study that received CSRT 2025 grant funding.