Introduction
Burns are among the leading cause of traumatic injuries in humans, corresponding to the fourth most common type of trauma worldwide, representing a major public health concern and contributing substantially to morbidity, mortality, and health-care costs.1,2 Burn injuries affect not only the physical health, but also the mental health and quality of life of the patients.3 Severe burn injuries often result in a systemic inflammatory response characterized by widespread cytokine activation, capillary leak, hypermetabolism, and immune dysregulation.3 These systemic alterations might eventually progress to multiple organ dysfunction, including hemodynamic instability, renal failure, and acute respiratory distress syndrome (ARDS).4–6
Inhalation injury, a serious pulmonary complication affecting 10%-20% of patients with burns, is one of the most critical determinants of outcome and an independent predictor of mortality. Mortality rates are as high as 50% in some series.7,8 The pathophysiology of smoke inhalation is multifactorial. Smoke inhalation causes lung damage through exposure to heat and toxic combustion products, with both local and systemic effects.9 Thermal injury predominantly affects the upper airway, leading to mucosal edema and potential airway obstruction. Meanwhile, exposure to toxic combustion products, such as carbon monoxide, hydrogen cyanide, aldehydes, and particulate matter, causes extensive injury to the tracheobronchial tree and alveoli.10 These toxins result in increased pulmonary vascular permeability and impair oxygen delivery through competitive bind to hemoglobin and inhibition of cellular respiration, metabolic acidosis and cardiovascular collapse.10
Inhalation injury damages both the upper and lower airways and can cause metabolic toxicity from substances such as carbon monoxide and hydrogen cyanide.11 Cellular damage triggered by products of combustion initiates an inflammatory cascade that leads to bronchorrhea, atelectasis, impaired mucociliary clearance, and respiratory failure while impairing immune function .12 These pathophysiologic changes significantly increase susceptibility to secondary bacterial pneumonia, making inhalation injury a major driver of ventilator-associated pneumonia (VAP) in burn patients.8,13
Consequently, inhalation injury is a major indication for mechanical ventilation (MV) in patients with burns, contributing to prolonged MV and increased hospital costs.14 Despite its recognized severity, the full impact of the contribution of inhalation injury to adverse outcomes, particularly VAP, remains incompletely understood. This study aimed to examine the clinical profile of patients with severe burn injuries and to evaluate the impact of inhalation injury on patient outcomes, especially focused on VAP and mortality.
Material and Methods
Study design and participants
This is a single-center retrospective cohort study conducted in a trauma center from January 2017 to December 2023. The Hospital de Pronto Socorro is a non-academic community hospital that serves as a referral burn center with 10 dedicated beds for the treatment of patients with burns.
We identified patients from the Hospital Infection Control Unit records, which contain records of all patients admitted to intensive care units (ICU). Eligible participants were all patients aged 18 years or older who had been admitted to the burn ICU with any degree of burn injury. Pregnant patients, patients admitted to the burn ICU for reasons other than burns or inhalation injury, and those with incomplete data were excluded.
Procedures
All procedures were conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki. The study protocol was approved by the institutional Research Ethics Committee (protocol number 7.076.879) on 14 September 2024. Informed consent was waived due to the retrospective nature and the anonymization of patient identifiers before analysis.
Clinical and laboratory data at ICU admission were collected from the medical records. Burn types were classified into fire, electrical, chemical, or thermal burns. Burns were graded as first, second, or third degree at ICU admission.6 The burn surface area was calculated at ICU admission as the sum of the second-degree and third-degree burn areas.15 Inhalation injury was defined as pulmonary injury resulting from inhalation of smoke or chemical products of combustion based on clinical signs and symptoms or bronchoscopy findings.9 VAP criteria included clinical suspicion (presence of fever, leukocytosis, and reduced oxygenation), the emergence of new or progressive radiological infiltrates, and a positive microbiological culture after 48 hours of initiation of mechanical ventilation.13 New cases of VAP were diagnosed based on the application of these criteria by the critical care team in charge of the patient and further adjudicated by the Hospital Infection Control Unit team. ARDS was based on clinical records according to the Berlin definition.16 Data on comorbidities, use of vasopressors, need for MV, duration of MV, need for prone positioning, rates of reintubation and tracheostomy, length of ICU and hospital stay, and mortality were also collected from the medical.
All patients were managed according to the same institutional standard of care and were subjected to standardized VAP prevention protocols, including standardized ventilatory management, head-of-bed elevation, routine oral hygiene, sedation and weaning protocols, and infection prevention practices as per institutional guidelines. All patients underwent respiratory therapy, which included bronchial hygiene techniques, such as changes in inspiratory and expiratory flow patterns, cough assistance, pulmonary expansion maneuvers, and airway aspiration using closed-systems techniques. Active mobilization and rehabilitation included sitting out of the bed, standing, and walking. The day on which each of these motor activities was first achieved was recorded.
Outcomes
The primary outcome was VAP incidence, analyzed exclusively in patients who were mechanically ventilated. Secondary outcomes included the need and duration of MV, ARDS incidence, need for prone positioning, rates of reintubation and tracheostomy, use of vasopressors, need for renal replacement therapy (RRT), length of ICU and hospital stay, hospital mortality, and comparison between survivors and non-survivors. The exploratory outcome included the time to begin active mobilization and rehabilitation (sitting out of the bed, standing, and walking).
Statistical analysis
To compare the VAP incidence between patients with and without inhalation injury, assuming a 20% higher rate in the injury group, a 5% significance level, and 80% power, the required sample size was estimated at 240 patients. Data were presented as mean (SD), median (IQR), or number (percentage). Comparisons between groups were performed using Student’s t test, Mann-Whitney U test, or chi-square test, as appropriate. Patients were divided into two groups: with inhalation injury and without inhalation injury. A Poisson regression model with robust error variances was used to estimate the relative risk (RR) of VAP, adjusted for age, burn surface area, and duration of MV. The impact of inhalation injury on the time to initiation of active mobilization and rehabilitation was analyzed using a log-rank test. The results were visualized with a Kaplan-Meier survival curve. For additional analyses, the patients were further divided into survivors and non-survivors. No missing data were imputed. Statistical analyses were performed using SPSS version 20.1 (IBM Corporation, Chicago, IL), and differences were considered statistically significant at p-values <0.05.
Results
Study population
From January 2017 to December 2022, a total of 245 patients met the eligibility criteria. Three patients were excluded because they were admitted to the burn ICU with other problems not related to burns or inhalation injury. Therefore, a total of 242 patients were included in the analysis. The baseline characteristics of the study population are summarized in Table 1. Briefly, most patients were male (72.7%) with a mean age of 44 (SD 17) years. The most common type of burn was fire (74.3%). Third-degree burns occurred in 64.0% of patients (n = 155). The median burn surface area was 23% (15%-37%). Fiberoptic bronchoscopy was performed in 13.2% of patients (n = 32). The incidence of inhalation injury was 9.9% (n = 24). The overall mortality was 22.3% (n = 54). Supplementary Table 1 shows biochemical profile of included patients at ICU admission.
Primary outcome
The overall incidence of VAP was 23% (n = 37) (Table 2). VAP incidence was significantly higher in patients with inhalation injury with an unadjusted RR of 2.1 (1.9-3.8) (p < 0.012). Since only intubated patients are at risk of developing VAP, only these patients (n = 161 – 137 of the group without inhalation injury and 24 in the group with inhalation injury) were included in the analysis of this clinical outcome. After adjustment for age, burn surface area, and duration of MV, the RR remained significant at 2.1 (1.2-3.7) (p = 0.009).
Secondary outcomes
The secondary outcomes are presented in Table 2. All patients with inhalation injury required MV (n = 24), whereas MV was needed in 62.8% (n = 137) of patients without inhalation injury (p < 0.001). The incidence of ARDS was similar in patients with and without inhalation injury (8.3% vs. 5.5%, p = 0.636). Among patients requiring MV, the duration of MV was 20 (3-32) days for patients with inhalation injury and 12 (4-23) days for those without inhalation injury (p = 0.463). This analysis refers exclusively to patients who were submitted to mechanical ventilation (n = 161 – 137 of the group without inhalation injury and 24 in the group with inhalation injury). Patients with inhalation injury had higher rates of reintubation (12.5% vs. 2.8%, p = 0.048) and tracheostomy (54.2% vs. 21.6%, p < 0.001).
The need for vasopressors (37.5% vs. 27.1%, p = 0.28) and RRT (8.3% vs. 13.3%, p = 0.748) was similar in patients with and without inhalation injury. Likewise, there were no differences in length of ICU stay (21 vs. 13 days, p = 0.249) or hospital stay (31 vs. 25 days, p = 0.663) between the groups with and without inhalation injury.
Table 3 compares survivors and non-survivors. The incidence of inhalation injury was similar in survivors and non-survivors (11.2% vs. 5.6%, p = 0.305). Likewise, the incidence of VAP did not differ significantly between survivors and non-survivors (13.3% vs. 22.2%, p = 0.108).
As expected, non-survivors had a higher burn surface area than survivors (40% vs. 20%, p < 0.01). The incidence of ARDS was higher in non-survivors (13% vs. 3.7%, p = 0.01) Additionally, non-survivors more frequently required vasopressor therapy (83.3% vs. 12.2%, p < 0.001), RRT (44.4% vs. 3.7%, p < 0.001), MV (98.1% vs. 57.4%, p < 0.001), and prone positioning (9.3% vs. 2.1%, p = 0.027) than survivors. Survivors had a longer length of ICU stay (21 days vs. 1 day, p < 0.001) and hospital stay (31 days vs. 1 day, p < 0.001).
Exploratory outcomes
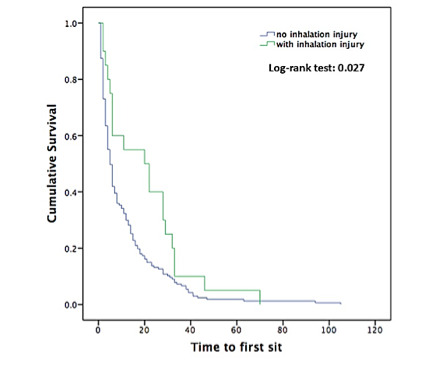
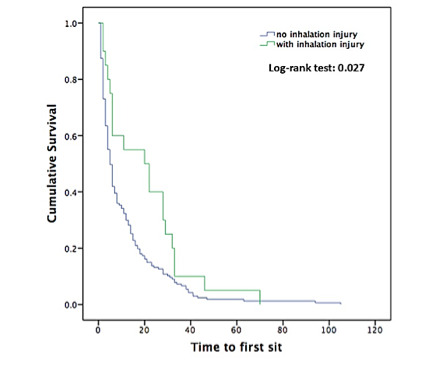
The day on which active mobilization and rehabilitation were first achieved differed between groups. Patients without inhalation injury experienced a shorter time to sit 5 (9-13) vs. 20 (13-28) days (p = 0.006) (Figure 1) and stand 9 (13-20) vs. 24 (14-33) days (p = 0.049) than those with inhalation injury. Additionally, there was a trend toward a shorter time to walk in patients without inhalation injury 12 (16-23) vs. 27 (16-35) days (p = 0.051).
Discussion
In this retrospective cohort of patients with burns admitted to a referral burn ICU, the incidence of VAP was higher in patients with inhalation injury than in those without inhalation injury. Despite this difference in VAP incidence, mortality did not differ between the groups with and without inhalation injury. Our findings show that inhalation injury independently doubles the risk of VAP, even after adjustment for age, burn surface area, and duration of mechanical ventilation. This indicates that inhalation injury contributes to pulmonary vulnerability beyond what can be explained by burn severity or ventilator exposure alone. In fact, inhalation injury should be viewed primarily as a marker of respiratory morbidity rather than mortality risk. While these patients require longer and more complex airway management, including higher rates of reintubation and tracheostomy, mortality appears to be driven predominantly by burn size rather than inhalation injury itself.
Burns not only affect the skin and mucous membranes on the body surface, but they can also lead to lung injury from smoke inhalation.4 Smoke inhalation injury occurs when fuel is burned indoors, leading to immediate death by suffocation or to the development of acute lung injury.11 In the current study, the incidence of inhalation injury was 9.9%, in line with previous reports showing an incidence of inhalation injury of 10%-20% in patients admitted to burn centers.7,8 However, incidences as high as 36% have been observed when inhalation injury is investigated by bronchoscopy.17,18 Direct laryngoscopy and fiberoptic bronchoscopy, the gold standard for the diagnosis of inhalation injury, can assist in the diagnosis by identifying early changes in the mucosa of the upper and lower respiratory tracts, such as erythema, edema, and pale mucosa that may not be evident on physical examination.19 Therefore, inhalation injury was probably underdiagnosed in our cohort because only 13.2% of patients underwent fiberoptic bronchoscopy, and its diagnosis is challenging based solely on clinical grounds. Moreover, a higher rate of inhalation injury was expected given the proportion of patients with second- and third-degree burns in our cohort, as the risk of inhalation injury increases with larger burn areas.20
Patients with severe burns seem particularly predisposed to develop VAP.18 The combination of severe thermal injury (systemic immunosuppression) and inhalation injury (local immunosuppression and tissue injury) creates an ideal environment for the development of VAP.7,21 Besides impairing pulmonary immune function, smoke inhalation induces cell injury, initiating an inflammatory cascade that leads to bronchorrhea, impaired ciliary clearance with formation of obstructive tracheobronchial casts, atelectasis, ventilation-perfusion mismatch, and hypoxic respiratory failure.7,8 Previous studies have reported an incidence of pneumonia of up to 50% in patients with inhalation injury requiring MV.22 We found an overall incidence of VAP of 15.3%, comparable to that of other general critically ill patients without burns.14,23 However, a 2-fold higher incidence of VAP was identified in patients with inhalation injury than in patients without inhalation injury. This incidence is consistent with the results of Shirani et al., who reported a 38.0% incidence of VAP in a cohort of patients with burns and inhalation injury, compared to 8.8% in those without inhalation injury.24 Although VAP was more common in non-survivors than in survivors, this difference was not significant. In the present cohort, burn degree, burn surface area, and organ failure were more important determinants of mortality than inhalation injury or VAP. Pneumonia is not an independent predictor of mortality in burns, but it significantly increases the duration of MV in patients with burns and inhalation injury.18,22 Although not significant, the median duration of MV was 8 days longer in patients with inhalation injury.
While mortality directly associated with smoke inhalation is relatively low (0% to 11%), it can be as high as 90% when combined with severe burns.25 Previous studies have shown that patients with burns and inhalation injury may experience up to a 10-fold increase in mortality compared with those without inhalation injury.26 However, in our cohort, mortality did not differ between groups. Although our sample size may be potentially underpowered to detect a difference in mortality, patients in our study were severely burned. Moreover, inhalation injury did not even have a negative impact on oxygenation early in the course of these patients. These features suggest that the extent of the burn surface area may have had a greater impact on mortality than inhalation injury itself. As we have previously demonstrated, the course of patients with inhalation injury was mainly determined by the percentage of burn surface area.27 Indeed, the burn surface area in non-survivors was twice that in survivors. Supporting this, Zhu et al. found that the burn surface area, along with other factors such as fluid requirements and MV, is an independent risk factor for mortality in patients with severe burns.28
Length of ICU and hospital stay, and duration of MV in our cohort of patients were longer than those in general ICU patients without burns and similar to those in patients with COVID-19.29,30 However, these findings are consistent with the literature on patients with burns.31 Despite no significant differences in the duration of MV between the two groups, patients with inhalation injury had higher rates of reintubation and tracheostomy. After inhalation injury, laryngotracheal stenosis may develop either due to mechanical trauma secondary to prolonged intubation or due to direct burn or irritation from inhaled smoke, chemicals, or other toxic materials. Such stenosis can lead to chronic damage to the airway, making the patient dependent on tracheostomy.32 Previous reports have shown similarly high tracheostomy rates, probably due to airway damage from inhalation injury.33 Moreover, patients with inhalation injury are often prophylactically tracheostomized to prevent airway obstruction.34
Active physical therapy plays a central role in the rehabilitation of patients with burns.3 Early interventions have been associated with better functional recovery after ICU discharge.35,36 The earlier physical therapy is started, the greater the benefit for movement.36 However, the majority of our patients had third-degree burns, hemodynamic or respiratory instability, and underwent multiple surgical procedures, precluding active mobilization and rehabilitation early in the course of their ICU stay. This highlights an important limitation to the application of established rehabilitation strategies in critically ill burn patients and might help to explain the observed outcomes.
This study included a 5-year cohort of consecutive patients from a referral burn ICU in a middle-income country, but some limitations should be noted. First, it is a single-center retrospective study. Second, fiberoptic bronchoscopy, the gold standard for diagnosing inhalation injuries, was not routinely used, which may have led to underdiagnosis. Nonetheless, this study comprises a large cohort of patients from a public burn center in Brazil, a resource-challenged environment for the diagnosis of inhalation injuries. Third, the diagnosis of VAP is difficult, especially in patients with other lung lesions. However, VAP incidence was independently adjudicated by the Hospital Infection Control Unit team. Fourth, the limited sample size might have obscured any association between inhalation injury and mortality.
Conclusion
The incidence of VAP was higher in patients with inhalation injury than in those without inhalation injury, but it was not associated with a higher mortality rate. Given the challenges in diagnosing VAP, particularly in the presence of inhalation-induced pulmonary injury, these findings heightened the need for VAP prevention, vigilance for early recognition of airway failure, and tailored ventilatory strategies in patients with inhalation injury. Besides, a more comprehensive investigation is warranted to clarify the distinct contributions of inhalation injury versus burn extent to outcomes.
Contributions
All authors contributed to the conception or design of the work, the acquisition, analysis, or interpretation of the data. All authors were involved in drafting and commenting on the paper and have approved the final version.
Funding
The authors acknowledge funding from Hospital de Clínicas de Porto Alegre (Tatiana Helena Rech, 10.13039/501100003810) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (Tatiana Coser Normann, 10.13039/501100002322).
Competing interests
All authors have completed the ICMJE uniform disclosure form and declare no conflict of interest.
Ethics
The study protocol was approved by the institutional Research Ethics Committee (protocol number 7.076.879) on 14 September 2024.
AI Statement
The authors confirm that no generative AI or AI-assisted technology was used to generate content.