Introduction
The SARS-CoV-2 pandemic created a major infection risk to clinicians in intensive care units (ICU) and infection control challenges that are ongoing and indicative of future risks. At the start of the pandemic, there was considerable uncertainty on how to mitigate risk to healthcare workers (HCWs) from direct exposure to the novel SARS-CoV-2 virus, especially during aerosol-generating procedures (AGP). Fortunately, guidelines to reduce AGP risk became available,1–7 but many gaps remained. In the ICU, there are indirect sources often unrecognized by clinical staff and potentially exposing HCWs and others to SARS-CoV-2 and other viruses. It is incumbent upon ICUs to develop and implement effective mitigation strategies to protect HCWs, visitors and patients. It is also vital to maintain the accurate performance of medical devices to ensure proper treatment delivery in such a situation and to monitor infection among healthcare workers during work.
There was little guidance on the safe and effective use of medical devices in the ICU during the SARS-CoV-2 pandemic, particularly for PICUs and NICUs. Appropriate concern by HCW that they were at risk also existed. To address this, at the onset of the pandemic, the neonatal (NICU) and pediatric (PICU) intensive care units of the Royal Children’s Hospital (RCH, Melbourne, Australia) took a proactive approach. They organized a small team with representatives from a range of disciplines—clinical technologists (staff with scientific and engineering backgrounds), medicine and nursing—to develop a comprehensive and practical response. We undertook a thorough and carefully considered process, supported by evidence when available, that was adaptable. The approach we report provided reassurance and confidence using clear, practical guidance not detailed before. It also assured our HCWs that their health and safety were the highest priority. Ultimately, it successfully managed and balanced risk, and we could continue uninterrupted patient care with zero known hospital-acquired spread of SARS-CoV-2 infection among staff at the bedside.
Material and Methods
Approaches Taken
At the beginning of the pandemic, we took a number of steps to identify and mitigate risks associated with the transmission of SARS-CoV-2 infection from patients to staff. We audited all respiratory equipment (excluding intubation equipment and bronchoscopes, which were covered by other guidelines) and processes for potential sources of contaminated gas, regardless of volumes involved, and sought guidance from suppliers and manufacturers as required (Table 1). We determined an appropriate mitigation strategy using an indirect approach to remove or replace the risk where possible (see Table 2) and a direct approach to filter gases using commercially available high-efficiency anti-viral/anti-bacterial filters (“filters” unless otherwise stipulated) or to scavenge gases using a high-pressure, high-flow vacuum regulator connected to hospital suction where possible (Table 3). We verified equipment performance with filters in situ and developed and implemented relevant procedures and practices.
Direct approach: filtering and scavenging
Supplier advice and filter choice
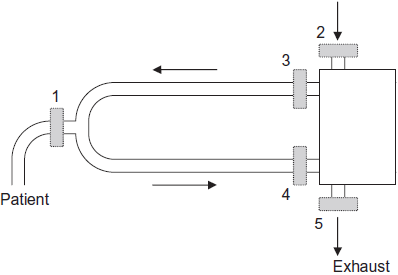
Ventilator manufacturers may recommend a filter suitable for use on their device to protect the patient and staff from contamination from infectious exhaled air, or users may need to select filters themselves either because of a lack of manufacturer’s recommendation or the inability to acquire the specific manufacturer recommended filter. Clinicians are then required to take reasonable steps to ensure that the chosen filters are fit for purpose. We assessed filter suitability based on both risk mitigation and the ability to properly provide therapy by considering deadspace (aiming for less than approximately 1/3 tidal volume4,10,13–15 to avoid rebreathing and increases in CO2), resistance to flow14 (aiming to avoid increasing work of breathing and inspiratory and expiratory time constants and to minimize the pressure drop across filters), viral filtering capability13,16 (to remove as large a proportion of SARS-Cov-2 viruses as possible along with any other bacteria and virus present), humidification capability and the compatibility with existing components (aiming to minimize additional connections, reduce the risk of disconnection and minimize stock holdings required). Where there was any uncertainty about the choice or use of a filter, advice was sought from suppliers/manufacturers. Figure 1 shows the various potential locations where a filter can be placed in a ventilator circuit, while Table 4 provides details of which filters we used and how we used them.

Bench testing
Selected filters were then tested in situ to ensure proper device operation, particularly if the use could be considered “off-label.”17 Ventilator bench testing was conducted to confirm proper device function with and without filters in place using the normal ventilator circuit(s) connected to a test lung (5601i, Michigan Instruments, Grand Rapids, MI, USA) with pressure and volume measurements taken using a separate respiratory monitor (NM3, Model 7900, Philips Respironics, Carlsbad, CA, USA). Manufacturer-recommended and local pre-use and start-up operating checks were performed, as well as operating the device over an appropriate clinical range of settings. Device performance was considered acceptable if all tests passed, performance was within manufacturer specifications, and set pressures and volumes were achieved without significant changes or loss of pressure and/or volume. In addition, alarm function was also assessed by the absence of additional alarms and the absence of significant additional delays in monitoring or alarm functions when filters were added. We found that all the ventilators and resuscitators tested were not affected by the presence of filters, and, in agreement with the manufacturer’s specifications, all filters only added a small pressure drop (≤2 cmH2O), even when multiple filters were required within a ventilator circuit. These pressure changes were all within the performance specifications of the ventilators and resuscitators and could be compensated for at the bedside. Any pressure drop caused by a filter on the inspiratory side is also irrelevant if proximal pressure monitoring is available (such as in the SLE5000 Infant ventilator [SLE Ltd, South Croydon UK]). Once it was determined that direct approaches to mitigating risk were possible, specific products were acquired and guidelines produced.
Filtering
Our primary approach was to pass all potentially contaminated gases through an appropriate filter. Some filter manufacturers gradually released statements confirming the suitability of their filters for SARS-2-CoV,18–20 and we liaised with suppliers to ensure that we had current information. We used filters for all suspected and confirmed COVID-19 cases and continued with standard practices in other patients. More widespread use of filters was employed at times of high local risk.
Filtration requires fewer connectors and components than scavenging, and filters are more visible and foolproof. There are potentially five locations (Figure 1) to place a filter in a ventilator circuit, the choice of which must balance risks to HCWs against complexity, cost, and deleterious patient effects. We accepted that we would need multiple filter types suitable for the different potential positions because supply could not be assured.13 Large, mechanical, pleated hydrophobic filters have the best filtration capabilities.13,16 They are suitable for placement within ventilator circuits where their large deadspace is not an issue. A patient size-appropriate filter is required when deadspace is relevant to clinical care. The relevant environmental risks we identified and the chosen mitigation strategies are summarised in Table 4. Details of our primary filters with photographs of them in use are detailed in Supplementary Table 1 and Figures 1-8.
We placed expiratory filters in the circuit before the expiratory port (i.e. position 4 in Figure 1) to avoid assuming that all exhaled gas exits from the primary outlet (the SLE5000 may leak gas from the exhalation block’s mechanical valve, for instance) and to avoid internal contamination rather than simply adding filters to the expiratory exhaust (i.e. position 5 in Figure 1).27 When placed like this, opening the circuit to replace the filter is necessary, which must be done cautiously and in appropriate PPE. It is ideally performed during routine care and when using hand-bagging as it allows the ventilator to be put into standby. The exhaust outlet should remain unobstructed, and close monitoring of the patient and ventilator pressure, flow and resistance5,6,10,17,26,28 and routine filter changes (24 hourly) are required as the resistance of any expiratory filter may increase or it may become obstructed.14
Some considered2,10,29 the Sensormedics 3100A/B high-frequency oscillator circuits (Vyaire, Yorba Linda, CA, USA) unsuitable in the pandemic as they have valves that may release gas before the exhalation port. Their design does not allow for filters to be readily added. The European Society of Paediatric and Neonatal Intensive Care (ESPNIC)2 recommends that for devices with free leak, such as the Sensormedics, a filter should be added to the expiratory limb and condensate collected in a closed system. It is insufficient to do this with the Sensormedics due to the multiple potential exit ports, but dedicated circuits with filters are available from Sensormedics (see Table 4) and were the circuits we used, although we utilized a conventional ventilator with in-built HFO where possible.2
Out of caution,13 we also added filters to the ventilator’s inspiratory outlet (Figure 1, position 3) as per manufacturer’s recommendations11,12,23 due to potential biofilm accumulation and passive ingress. Inspiratory filters are changed at longer intervals (typically seven days) than expiratory filters (24 hourly),30 which helps manage stock levels. Standardizing filters for as many applications as possible is also advantageous. Having the same filter on both inspiratory and expiratory ports is also safer, as erroneously omitting the expiratory side should be avoided.13 It has also been suggested13 that using two filters in series can create some redundancy and increase filtering, but we did not do this. Kits were made to make it quick and easy to install appropriate filters (see Supplementary Table 2).
Some ventilators, such as the Hamilton C1 (Hamilton Medical AG, Bonaduz, Switzerland), also draw in room air that is delivered to the patient, so it is important that appropriate filters, such as HEPA filters12,31 are in place (i.e. Figure 1, position 2) to filter potentially contaminated room air before it is added to the ventilator gas flow.
While it has been suggested that filters be left out of manual ventilators for small neonates,10 we used them. We added the filter between the Ayre’s T-piece or Neopuff circuit and endotracheal tube with the deadspace managed as required. To avoid adding deadspace, the filter could be moved into the Ayre’s T-piece circuit13 distal to the patient connector (see Supplementary Figure 7), but this potentially allows contaminated gas to travel up the oxygen or manometer tubing and is not possible in typical self-inflating resuscitators or on some neonatal resuscitator circuits.
HMEFs, as opposed to HMEs, can be used in dry circuits at the endotracheal tube (ETT) (i.e. Figure 1, position 1) to provide humidification as well as filtering and preventing circuit contamination but are contraindicated in the presence of active heated humidification.4–6 Smaller filters, such as pediatric HMEFs, typically do not have as good filtering characteristics as larger mechanical, pleated types, so it is advisable to also have larger mechanical, pleated types at the ventilator’s inspiratory and expiratory outlets.13 We used standard heated humidification but used HMEFs for peri-hospital transport.
A potentially overlooked risk is the contamination of ETCO2 and NO monitoring equipment and its exhaust. This can be avoided by sampling after an appropriate placed filter if possible13,14 or using a 0.2µm drug injection filter on the monitoring line.13 We found adding a filter between the sample line and device was possible for NO monitoring but was not ideal for ETCO2 monitoring because the added resistance and volume of the filters affected the pump and time response, so we collected the ETCO2 exhaust gas with scavenging13 and only when ETCO2 was required for transport was a filter (BB50) added. We also, particularly in NICU, moved from ETCO2 monitoring to transcutaneous monitoring for COVID-19-positive or suspected patients whenever possible to avoid potential issues with ETCO2.
Scavenging
We have an established system for routinely scavenging nitric oxide (NO). While a first-line option for some,27 or used in conjunction with filters by others,29,32 scavenging was our secondary option (see Supplementary Table 3) and a backup if we were unable to access sufficient filters. Although the scavenging system is relatively simple, the extra components and suction regulators made this more resource-demanding and prone to potential limitations, including being turned off, having inadequate flow or being obstructed. It was important, however, to ensure that suction did not affect the device’s operation and that pressure (negative from over-suction or positive from loss of suction and build-up of exhaust gas) could not be generated and applied to the device by using a tee piece with an unobstructable open port (see the Supplementary Figure 8B for example).
Incubator use
Incubators were commonly recommended for use during the pandemic for transport and care of babies,3,10,33–35 although they do not provide the same level of protection as negative pressure rooms or air filtration36 and their exhaust flow is an additional source of potential contamination. ESPNIC3 recommends minimizing heating and/or humidification within the incubator to minimize aerosol spread and placing the neonate in a plastic bag, covering the incubator’s portholes to minimize leakage. Connecting suction in order to create a mini negative pressure room has also been reported.37 Air circulated inside our Drager fleet of incubators and hybrid devices constantly leaks out from multiple locations, such as around the canopy, ports and grommets,38 so we were unable to filter or scavenge it, but we did use them as a physical layer of protection where possible.
Staff surveillance and work-related infection
Our hospital ran an extensive staff infection detection and surveillance program during the pandemic, including the NICU and PICU. This was overseen by our Infection Prevention and Control Department. This included pre-shift health questionnaires and declarations for all staff regarding health and COVID status and exposure, SARS Co-V2 PCR and rapid-antigen testing, identifying potential exposures and contacts and furloughing exposed staff. All staff who tested positive for COVID were identified through this process and followed up to identify potential exposures and/or contacts with COVID-positive or high-risk patients or visitors. These precautions were performed in conjunction with our other risk mitigation strategies, such as the use of Airborne precautions and appropriate PPE use, appropriate building design and air conditioning, the use of predominantly single patient rooms, visitor restrictions and screening and the cohorting of COVID positive and suspect COVID patients.
In the PICU and NICU, there are over 500 staff members. There were 4,500 COVID-19 infections throughout the hospital among HCWs and other staff, with a peak of 650 staff per month hospital-wide acquiring COVID-19 infection from the community. During three years of intensive surveillance, we recorded zero infections confirmed or suspected as being acquired from patients among our NICU and PICU teams of HCWs.
Discussion
At the beginning of the pandemic, there was a great deal of concern and undetermined risks faced by HCWs and a lack of practical guidance. A proper response was required to provide confidence and practical solutions to the risk mitigation issues raised. We developed an original and useful process to identify and mitigate the risk of breathing contaminated gases to HCWs, visitors, and patients that others can adapt in different locations and situations. We feel that the novelty and value of our work is establishing a detailed process to thoroughly evaluate needs and options and enact a range of appropriate mitigations. These needs are infrequently described in detail, particularly in the PICU and NICU setting. The key aspects of our mitigation were the appropriate use of filters with the additional use of scavenging as required with a thorough device performance evaluation. The risk mitigation undertaken is a balance between absolute risk mitigation to staff, visitors, and patients versus the effectiveness of the treatment we want.
The initial steps we undertook consisted of auditing our equipment and processes to identify risk, seeking advice from suppliers/manufacturers and devising mitigation strategies using indirect and direct approaches, largely filtering. Importantly, we then performed tests on equipment to verify proper function and the absence of negative impacts when filters and/or scavenging was used, and this was done with ongoing liaison with suppliers/manufacturers. As detailed in the “bench-testing” section of the Materials and Methods above, bench testing of ventilators and resuscitator was performed with and without filters in situ to confirm proper functional performance, alarm behaviour and monitoring. This consisted of ensuring the passing of pre-use tests and the achievement of set pressures and volumes without significant changes or loss with and without filters in place, ensuring the proper functioning of alarms, the absence of additional alarms and the absence of significant additional delays in monitoring or alarm functions. Even with multiple filters in place, we found that filters only added small but acceptable pressure drops that were within the performance specifications of the ventilators and resuscitators and could be readily compensated for in clinical use.
To enact the necessary new approach, we developed and implemented relevant procedures and practices. We also found that it was important to utilize the experiences of others and the existing knowledge from the management of other infectious patients. Still, it was particularly useful, and an option that others may not have access to, to have a multidisciplinary team guiding the process.
Filtering gas with appropriately sized, placed and performing filters is the key step in protecting from contaminated gases. It is vital that the locations that contaminated gas can exit the ventilator and associated circuits are identified and filters located appropriately. Reducing the viral burden released into the room is important.39 HMEs and filters have long histories in anesthesia and intensive care14,16 but there is little specific literature about the placement of filters for ventilated patients, possibly because the topic is considered established practice and knowledge assumed. Textbooks for instance,40 recommended using a HEPA filter on all exhalation from mechanically ventilated patients in the influenza pandemic, and ventilator manufacturers routinely recommend their use. Unfortunately, despite their somewhat ubiquity, knowledge of the proper use of filters is incomplete and specific guidance like the one we describe is required. Further, the uniqueness of the COVID-19 pandemic required many to question whether existing practices were adequate for reducing inadvertent viral exposure.
Our approach is consistent with reports in adult ICU and anesthesia during this pandemic. Lucchini et al.27 recommend the use of helmet CPAP with a HEPA filter, active scavenging to the ventilator gas outlet and HEPA filters if scavenging is not available, HME and HEPA filter between patient and ventilator circuit for transport and HEPA filters between the manual resuscitator/T-piece connector and patient. Sorbello et al.41 advised the use of a “HEPA filter on every oxygenation interface” and recommended a HEPA filter between the airway and ventilator circuit, including the expiratory limb of the circuit, based on experience gained during the SARS pandemic42 but provided little additional specifics pertaining to filters. Wax et al.43 also did not provide many filter details but recommend the use of filters for CPAP/BIPAP, bag-mask ventilation and for all ventilator exhaled gases in adult ICU and suggest the use of a filter on the exhaled port of an oxygen rebreather mask but mention that the infection control efficacy of this is not established. To our knowledge, our report is possibly the first to address gas filtering and scavenging in NICU and PICU.
Some NICU and PICU organizations have published recommendations for managing risks to HCWs. The European Society of Paediatric and Neonatal Intensive Care (ESPNIC)2,3 recommends helmets for NIV or, if unavailable, a ventilator with a dual limb circuit and filter (or single limb with filter before the leak), a self-inflating resuscitator with a filter and two-person technique to improve mask seal, and the use of a filter on the expiratory limb of ventilator circuits and, for non-turbine ventilators, the use of a filter on the inspiratory side. The Paediatric Intensive Care Society (PICS)4–7 recommends using a bagging circuit with a filter and aiming exhaust away from staff, using disposable ventilator circuits, “protecting” ventilators with a filter and avoiding ventilator disconnections. It has also been commonly recommended to nurse COVID-19-positive or suspected babies inside incubators.2,3,35,36
In a review of respiratory care of neonates during COVID-19, Shalish et al.10 recommended placing a filter in the expiratory limb for CPAP and NIV, between the patient and self-inflating resuscitator and, for mechanical ventilators, before the expiratory valve but never between the circuit adaptor and endotracheal tube (ETT). Filters in ventilator circuits are not mentioned in the review of Ong et al. of COVID-19 in PICU44 but they recommend using a filter with self-inflating resuscitators, although manual ventilation should only be used if necessary and with small tidal volumes and a tight mask seal. Ma et al.34 and Wang et al.32 recommend placing a head cover connected to scavenging over suspected neonates and adding filters to self-inflating resuscitators and filters connected to scavenging32 to the expiratory end of the ventilator. Cavicchiolo et al.33 do not mention the use of filters in their NICU, while Thampi et al.45 suggest avoiding bagging in PICU/OR but using a filter and small volumes if required and using hydrophobic mechanical filters on the inspiratory and expiratory limbs of ventilators. There are also some recommendations from PICUs in resource-limited settings46 to use oxygen hoods during HFNC or bubble CPAP and dual limb NIV circuits with filters (or filters on exhalation port if single limb used) and filters on ventilators and self-inflating resuscitators. Locally, guidelines from the Australian and New Zealand Intensive Care Society (ANZICS)1 recommend closed circuits with filters on ventilators and on self-inflating resuscitators but provide little specific guidance.
Experience with the SARS pandemic also provides some additional, relevant guidance. Hui47 warned to “be aware of air leakage from the various respiratory therapies.” Kamming et al.42 and Fowler et al.48 recommend the use of filters between the patient and self-inflating resuscitators and on the expiratory limb of the ventilator circuit. Ng et al.29 used filters on resuscitator bags and added filters as well as scavenging to the expiratory port of their ventilators and managed all high risks neonates inside incubators, with patients on CPAP also inside a headbox connected to scavenging inside the incubator, and minimized leaks from incubator portholes.
There were also some other standard care practices that we addressed. We routinely clamp endotracheal tubes in various circumstances, including to maintain lung volume and required disconnections. We routinely applied that practice to COVID and COVID-19 suspected patients to minimize any potentially contaminated exhaled air entering the room for any disconnection of the ventilator circuit based on basic principles and the recommendations of others.4,5,27,41 We also used closed inline suction catheters that had a valved one-way lavage/cleaning port to avoid any patient exhaust/spray and considered this a low-risk but necessary procedure managed by minimizing the time taken to disconnect or with open circuits and, importantly, with general precautions in place (including PPE).
The available guides and publications provided limited useful, practical guidance, so we went back to basics and developed what we think is a novel approach to assessing the situation, determining a course of action and safely and effectively implementing it. It would be an oversimplification to think of our process as just adding filters. While that was the major physical intervention we carried out, it was supported by, and only successful because of, the conduct of the other steps – auditing risk, reviewing options, testing options, and ultimately introducing the proper application and procedure. The value of the process we undertook was in its thoroughness and practicality and its eventual success at balancing risk with the ability to provide suitable treatment.
Conclusion
The appropriate use of filters and/or scavenging to mitigate the risk to HCWs, visitors and patients in the presence of infectious patients is a small but vital part of a broader approach required to manage patients with COVID-19 and keep HCWs and others safe.1–7,10,27,32–34,41,43–45 We have now utilized the approach detailed here in our NICU and PICU for the last three years while managing children with both suspected and confirmed SARS-CoV-2 infection, as well as during potential local outbreaks within the ICUs. The system has been successful as we have been able to continue offering all desired care to our patients, and we are unaware of an HCW acquiring an infection from a patient. Maintaining stock and use of the filters and the approaches detailed here provide an approach that can be applied beyond the current COVID-19 pandemic. We have focussed on presenting the process and considerations we made to determine our practices to provide a framework for others to adapt to their local conditions during current and future pandemics and local viral outbreaks.
Acknowledgment
We would like to acknowledge the assistance of other members of the Clinical Technology Service for testing and support, as well as other members of the PICU and NICU COVID-19 response teams for their efforts in meeting the challenges of this pandemic.
Contributors
BC, EH and DT contributed to the conception of the work while all authors contributed to the acquisition, analysis, or interpretation of the data and were all involved in drafting and commenting on the paper and have approved the final version.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval
Not required for this article type.