Introduction
The coronavirus disease 2019 (COVID-19) pandemic stressed our healthcare system.1,2 During the pandemic’s initial phase, approximately 25-30% of patients developed acute respiratory distress syndrome (ARDS), requiring invasive mechanical ventilation (MV) and admission to the intensive care unit (ICU).3–5 ARDS carries a high mortality and morbidity rate with no definitive treatment.6 Lung protective MV, prone positioning, and the promotion of ventilator synchrony through sedation and paralytic agents improve ARDS outcomes, primarily by preventing further iatrogenic lung injury.7,8
Respiratory therapists (RTs) specialize in cardiopulmonary care and form a surveillance system to detect subtle changes in respiratory status.9,10 Most states in the United States require RTs to pass a credentialing exam to verify their ability to fulfill this specialized role. The National Board for Respiratory Care, which confers credentials, requires candidates to be graduates of an accredited education program. The accreditation standards for entry-level RT education programs require a minimum of an associate degree.11 In 2016, the American Association for Respiratory Care (AARC) revised a position statement to require new entry-level programs to award the baccalaureate degree.12 The Commission on Accreditation for Respiratory Care (CoARC) accreditation standards followed and specified a baccalaureate degree for new entry-level programs in 2018.13 Later, the AARC targeted 2030 as the date for an entry-level baccalaureate requirement citing the need for increased critical thinking skills, higher success rates of baccalaureate graduates on credentialing exams, and preferences from RT managers.13,14 However, beginning in January 2022, the CoARC reversed its earlier decision to require a baccalaureate degree for new entry-level programs to avoid the exacerbation of a workforce shortage. The CoARC also cited the lack of empirical evidence supporting advanced education for professional practice.15
The nursing profession explored how advanced education enhanced their professional practice through two decades of research across multiple care settings. Consistently positive results emerged when a greater percentage of nurses with baccalaureate degrees or higher provided care.16–23 To date, there is a lack of studies that suggests RTs with baccalaureate-level degrees affect patient results. The COVID-19 pandemic provided a natural experiment for evaluating how the academic degrees of RTs influenced discharge outcomes. Therefore, this study addressed whether RTs with advanced degrees affected the discharge outcomes and length of stay for patients with COVID-19 pneumonia requiring MV. A secondary aim addressed the role of RT adult acute critical care competencies on the same outcomes.
Study Design and Methods
Study Design, Setting and Subjects
This retrospective, cross-sectional study was conducted among subjects who received care in March-May 2020 at a Midwestern academic medical center that used RT-driven protocols. The local institutional review board approved the study protocol (ORA#20063001). Adult subjects with a confirmed or suspected COVID-19 diagnosis, admitted to the hospital for at least three days and received MV, were included. Pregnant subjects were excluded to eliminate the impact of pregnancy-related complications.
Measures
Subjects’ demographic data was obtained from the electronic medical record (EMR), including age, sex, primary race, and body mass index (BMI). We measured race because early findings found a higher incidence of COVID-19 in marginalized communities.24 Indicators for illness severity included comorbidities, sequential organ failure assessment (SOFA) score and PaO2/FiO2 at MV initiation. Protocolized RT interventions included prone sessions, plateau pressure (Pplat) >30 cm H2O, and spontaneous breathing trials (SBTs). We recorded the academic degree of the RT who assessed the patient immediately prior to the first prone session and who recorded Pplats >30 cm H2O and SBTs. Lastly, the time (hours) from intubation to the first prone session and the subsequent number of prone sessions were recorded. The institutional protocol specified proning anytime the PaO2/FiO2 fell below 150. The proning team consisted of 4-5 members, including nurses, nursing assistants, occupational therapists, physical therapists, and RTs. Frequencies of Pplat greater than 30 cmH2O were recorded. Additional data included lengths of ventilator, ICU and hospital stays, and hospital discharge dispositions. Descriptive data from personnel files were extracted for each RT name in the EMR associated with a patient ventilator assessment. Data included the highest academic degree (baccalaureate degree or higher vs. associate degree), years of RT experience, Adult Critical Care Specialist (ACCS) credential, and completion of adult critical care competencies. Adult critical care competency testing addressed an ARDS scenario and included patient assessment, acid-base analysis, chest radiograph interpretation, ventilator management, and ventilator waveform interpretation. Competency testing occurred during employee orientation and annually thereafter, requiring employees to achieve a competency score ≥75% to provide critical care. However, to facilitate staffing during the pandemic’s surge, the department waived this competency requirement for temporary RT staff and graduate-degree RT students (within one semester of graduating). The institution targeted a staffing ratio of six intubated patients per RT.
Study Outcomes
Study endpoints were the impact of RT advanced degrees and adult critical care competencies on the subject’s discharge status and lengths of stay. Discharge outcomes were considered good, compromised, or poor when subjects’ hospital discharge was directly to home, long-term care facility/rehabilitation center, or hospice/died, respectively. Length of stays were the durations (days) of MV, ICU, and hospital stays.
Statistical Analysis
Descriptive statistics for categorical variables were reported as frequencies and continuous variables as means and standard deviations or as medians and interquartile ranges (IQRs). The differences between the groups were evaluated using the 2-tailed t-test, Mann-Whitney test or Kruskal Wallis test, for quantitative variables and the chi-square test or Fisher exact test for categorical variables and tested at α=.05.
Multi-state Models
Model 1 was a time-to-event, four-state regression model assessing the impact of RT and patient covariates on three hospital discharge outcomes.25–27 The model’s states were the baseline (intubated), good, compromised, and poor states allowing for three possible transitions from the baseline to either of these three discharge states. Model 2 was a time-to-event, three-state regression model evaluating the impact of RT and patient covariates on ventilator and ICU outcomes. Model 2’s states were baseline (intubated) and binary transition states of either good (alive) or poor (died or hospice discharge). A sensitivity analysis was used to establish the optimal threshold for the two primary covariates used in both models; RT academic degree and adult critical care competencies. For both RT covariates, a subject-level variable was assigned a 1 to subjects who had more than 85% exposure time to RTs with advanced degrees or those who completed adult critical care competencies; 0 to other subjects. The exposure time >85% was selected because it yielded the highest effect size for the advanced degree. Subject covariates (SOFA, hypertension, BMI, and age) were included based on bivariate analyses and prior research. Missing SOFA data points were inputed using the SOFA score median. BMI and age were used as continuous covariates, and hypertension as a nominal variable. The multi-state model integrated covariates through Cox proportional hazards regression using R’s mstate package, version 4.0.3.28,29 Other analyses were conducted using SPSS, version 26.0.
Results
This study included 260 subjects with a median age of 59 y (IQR 49-68) (Table 1). Of these, the median BMI was 31.4 (IQR 27-38), 166 (63.8%) were males, and the primary race was African American for 98 (37.7%) subjects. The median SOFA score was 4 (IQR 3-5), and median PaO2/FiO2 was 235 (IQR 191-305). RTs proned 197 (75.8%) subjects, with the medians for prone sessions being 2 (IQR 1-4) and time to first prone session 10 hours (IQR 5-44). RTs recorded SBTs in 158 (61%) subjects for a median of 1 (IQR 0-3). Of 260 subjects, we found good discharge outcomes for 36 (13.8%), compromised for 118 (45.4%), and poor for 106 (40.8%) subjects. There were no differences in age, gender, BMI, or primary race among discharge statuses. Hypertension was more prominent in the compromised and poor groups (p=.021), and PaO2/FiO2 was lower in those with poor outcomes (p=.003). The poor group had a significantly higher SOFA score (p=0.043), received more frequent prone sessions (p<.001), and less frequent SBTs (p<.001). The compromised group spent more days on the ventilator, in the ICU, and the hospital as compared to the good and poor groups (p<.001).
The 260 subjects admitted during the study period received care from 132 RTs (46 permanent RTs, 81 temporary RTs, and five graduate-level student RTs), had a total of 29,961 RT encounters, and averaged 115 RT encounters per subject (Table 2). Median RT experience was six y (IQR 3-11), with 45.8% holding master’s degrees, 28.1% associate degrees, 24% bachelor’s degrees, 0.9% Ph.D. degrees, and 1.1% RT students. Furthermore, 70.8% of RTs completed adult critical care competencies, and 52% held the ACCS credential. RT experience was similar across all discharge outcomes. However, a between-subjects evaluation showed that subjects with good outcomes encountered fewer RTs with advanced degrees and more RTs with adult critical care competencies and ACCS certification (Table 2). There was a significant association between RTs with adult critical care competencies and ACCS certification (p<.001).
Regarding proning, no significant differences emerged across study groups related to RT education attributes of RTs providing respiratory care immediately prior to proning. However, when survivors (good and compromised outcomes) were compared with those who died, care immediately prior to proning from an RT with an advanced degree favoured survival, p=.038. Compared to those with compromised or poor outcomes, subjects with good outcomes received care more frequently from an RT with critical care competencies, p=.041. The frequency of Pplat values >30 cm H2O increased among compromised and poor groups as compared to the good group (p<.001). When comparing discharge outcomes, RTs with advanced degrees recorded Pplat >30 cm H2O more frequently in the good discharge group (p=.004). Adult critical care competencies had no impact on the recorded Pplat (p=.133). RTs recorded a total of 459 SBTs among all subjects, of which RTs with advanced degrees recorded 289 (63%) and RTs with critical care competencies recorded 357 (78%) SBTs. When assessing SBT performance between the quality of discharge outcomes, RT degree had no impact (p=.063). However, RTs with critical care competencies performed SBTs more frequently in the good outcome group (p=.019).
Table 3 shows how different thresholds of each subject’s exposure to RTs with advanced degrees and adult critical care competencies yielded a good discharge status. A >75% subject exposure to RTs with advanced degrees had no significant impact on good discharge status compared to less exposure (p=.12). However, subjects with >80% exposure to RTs with advanced degrees transitioned 2.47 times more frequently to a good discharge status (p=.005). At 85% exposure, the transition frequency was 3.72 times higher (p< .001). Similarly, increased subject exposure (>80%) to RTs with adult critical care competencies yielded significantly higher transition rates to good discharge outcomes.
Study Outcomes
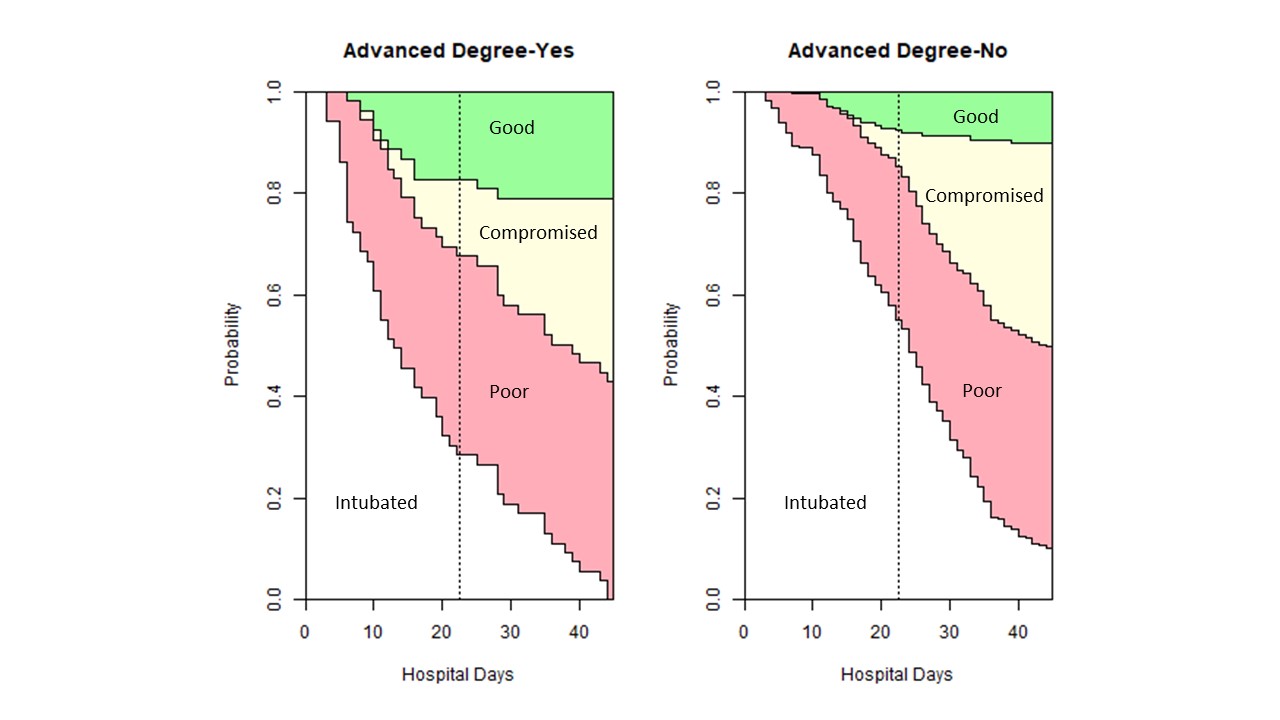
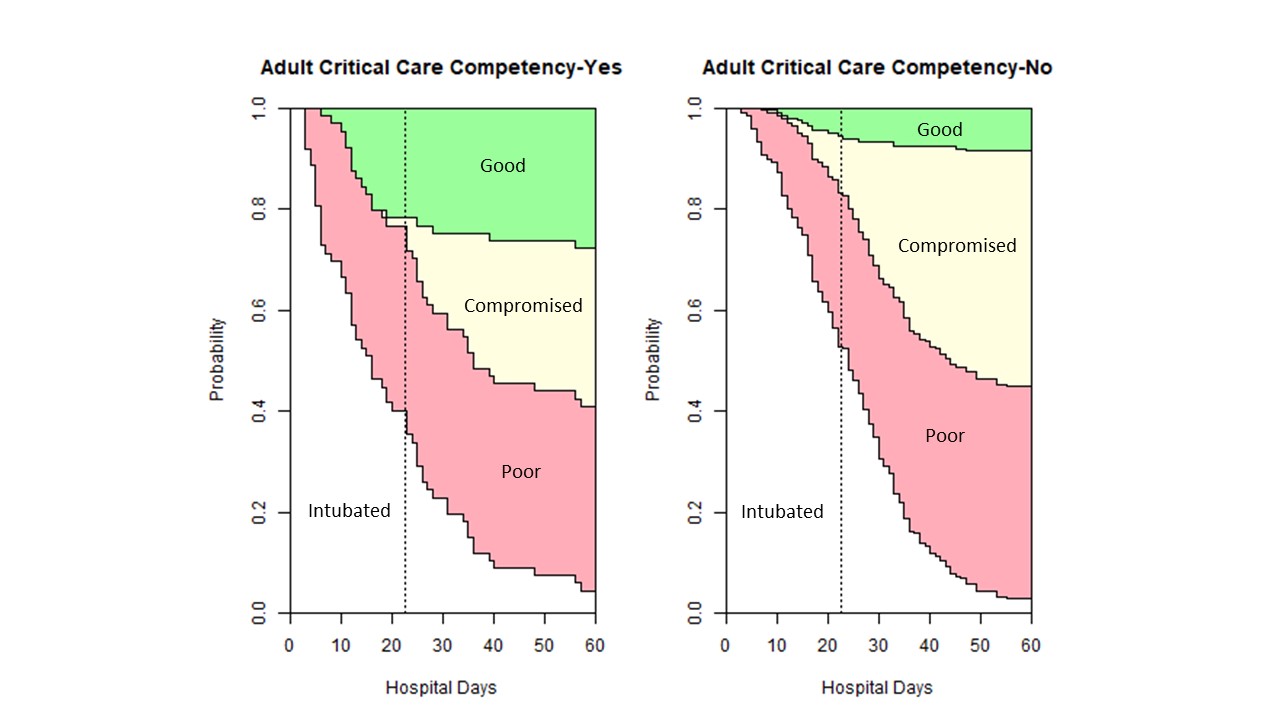
The time-to-event multi-state model (Model 1) demonstrates the impact of RT education, RT competencies and patient characteristics on discharge outcomes (Table 4). When evaluating hospital stay, each subject with >85% exposure to RTs with advanced degrees transitioned 3.72 (95% CI 1.75-7.91) times more frequently to the good outcomes as compared to those with less exposure (p=.001). Figure 1a shows that among subjects with >85% advanced degree RT exposure at hospital day 22 (median value), the probability of transitioning to a good outcome was 18% as compared to 8.1% with less exposure. Similarly, subjects with >85% exposure to RTs with adult critical care competencies transitioned 5.10 (95% CI 2.54-10.24) times more frequently to the good outcome compared to those who did not (p<.001). Figure 1b highlights how subjects with >85% exposure to RTs with adult critical care competencies at hospital day 22, the probability of transitioning to a good outcome was 23% as compared to 6% with less exposure. The SOFA score had a mild impact on the hospital discharge outcomes leading to a 1.12 transition rate towards death, p=.046. However, subjects with hypertension transitioned less frequently to the good outcome (p=.018) and nearly half as frequently to the poor outcome (p<.001). Furthermore, subjects with higher BMI transitioned more frequently to the compromised (p=.004) and poor (p=.005) states. Persons with advanced age transitioned 1.03 times more frequently to the poor state (p=.021). An >80% RT exposure threshold showed consistent findings with weaker magnitude, see Supplementary Data, Table 1.


Results from Model 2 appear in Table 5. When evaluating ventilator days, subjects with >85% advanced degree RT exposure transitioned 1.72 (95% CI 1.21-2.45) times more frequently to good discharge outcomes (p=.002). Similarly, subjects with >85% exposure to RTs with adult critical care competencies transitioned 1.94 (95% CI 1.36-2.75) times more frequently to good outcomes (p<.001) and 2.60 (95% CI 1.46-4.63) times to poor outcomes (p=.001). Subjects with higher BMI (p=.002) and advanced age (p=.04) transitioned more frequently to the poor outcome.
When assessing ICU days, subjects with >85% advanced degree RT care and >85% adult critical care competencies exposures transitioned more frequently to good discharge outcomes, 1.90 (95% CI 1.35-2.68) times (p<.001) and 1.78 (95% CI 1.30-2.46) times (p<.001), respectively. Subjects with advanced age and higher BMI were significantly more likely to transition to the poor state.
Discussion
This is the first study to explore the impact of either advanced RT academic degrees or critical care competencies on patient outcomes. Findings show that RTs were heavily involved in providing care to patients with COVID-19 pneumonia receiving MV, averaging 115 assessments per patient. Furthermore, the findings revealed that patients with greater than 85% exposure to RTs with either advanced degrees or critical care competencies were more likely to be discharged home.
Mortality rates of 30-50% occurred when patients with COVID-19 pneumonia required MV,30–32 which matches this study’s 40.8% hospital mortality rate. Higher mortality is associated with advanced age, obesity, and poor oxygenation.31 Additionally, ARDS clinical outcomes depend on the timely application of guideline-based ventilator management and prone positioning.7,8,32,33 A study evaluating ARDS management in patients with COVID-19 reported that only 50.4% of patients received ARDS guideline-based clinical management, though RT characteristics were absent.34 In the United States, RTs serve as the surveillance system for identifying the need, adjustments, and ongoing monitoring for lung-protective strategies, prone positioning, and others. Thus, exploring the relationship RT characteristics have on clinical outcomes is essential.
The nursing profession studied how educational characteristics affected patient outcomes and found that a 10% increase in nurses with baccalaureate degrees reduced 30-day mortality by 4%-8%.19–22 A greater impact of advanced nursing education on mortality odds occurred in postsurgical patients with dementia highlighting how the problem-solving and synthesis skills of more highly educated nurses benefit vulnerable patients who cannot communicate.23 Further, longitudinal changes in patient safety and quality care measures made over a decade showed that increases in the percentages of nurses by 10% reduced the odds of unfavourable safety and quality ratings between 7% and 17%.34 A Canadian study found patients with acute illnesses had lower rates of 30-day patient mortality when cared for by nurses with a baccalaureate degree [OR 0.81 (95% CI 0.68-0.96)].16 Another Canadian study explored mortality outcomes from adults with medical illnesses and reported that a 10% increase in the proportion of nurses with baccalaureate degrees resulted in a 9% reduction in mortality.17 In critical care settings, each 10% increase in the number of nurses with baccalaureate degrees lowered the risk of mortality by 2% in adults receiving MV.35 Given RTs’ surveillance responsibilities for a complex therapy like MV, the impact of care received from RTs with advanced degrees on mortality in the current study is unsurprising. Regarding the respiratory therapy profession, the stacked probability figure (Figure 1) suggests that RT advanced education aided discharge to home in fewer days. Although it is difficult to identify how a single profession affects a patient’s outcome, this study explored the association between RT education and specific RT protocol interventions such as proning, Pplat management, and SBT. A positive survival outcome was associated with receiving care from an RT with an advanced degree immediately prior to the first proning session. Between subjects, our data revealed that RTs with advanced degrees were more likely to record Pplat >30 cm H2O. This unexpected finding may be attributed to the study methodology. We pulled Pplat values from the patient’s chart but did not individually audit whether a high value was recorded and immediately followed by a ventilator change to align with the institution’s lung protective protocol. A closer audit process is needed to confirm future results. Academic degrees did not affect the overall SBT frequency among discharge outcomes. The retrospective nature of the analysis makes definitive conclusions difficult.
Patient mortality is an important metric; however, health status on discharge also matters. A recent study exploring outcomes from inpatient cardiac arrest found a 10% increase in nursing staff with baccalaureate degrees led to increased odds of surviving with good cerebral performance [OR 1.24 (95% CI 1.08-1.42)]. When only survival outcome was explored, nurse education was not significant.36 The current study similarly addressed the quality of the discharge status. Our study showed that when >85% of care was provided by RTs with a baccalaureate degree or higher, the transition to home was almost 4 times the rate compared to less care provided by RTs with an advanced degree. Some may argue that work experience is an adequate substitute for advanced education. Several studies in the nursing literature refute that argument.19,21,22 In the current study, work experience was not associated with improved patient outcomes.
The nursing profession recognizes education and certifications as part of the Magnet program.37 Specific to Magnet’s scientific discovery value, the impact of a baccalaureate degree on evidence-based practice was studied, and nurses with baccalaureate degrees had greater desires, ability, and frequency of using evidence-based practices.38 Nurses are the first line of surveillance for detecting healthcare complications because of their proximity to the patient and contact time.39 Similarly, RTs play an important surveillance role for patients requiring MV and also need evidence-based practice structures. Like Magnet, the AARC has recognition for respiratory care excellence in acute care hospitals through the Apex Award. Amongst the award’s criteria, the RT department must conduct annual competencies for all RTs, and at least half of the RT staff must have a bachelor’s degree.40 The current study was conducted at a facility holding the Apex designation and may support the positive impact of education and competencies on patient outcomes. However, further investigation is needed since only one Apex department was studied.
In 1992, the Evidence-Based Medicine Working Group published an article that emphasized the use of evidence-based clinical practice to improve patient outcomes.41 Competency-based education has been used since in both pre-professional education and ongoing clinical education to teach evidence-based clinical practices.42,43 A study that evaluated the impact of competency education among nurse practitioners and physician assistants showed significant improvement in acquiring new knowledge and skills.44 Another study explored the impact of competency-based education on resident physicians’ learning related to MV and reported an increase from baseline 31% to 96% in residents’ ventilator management confidence.45 Critical care competencies in the current study also appeared to impact discharge outcomes. Patients requiring proning had better discharge outcomes when the RT who provided their respiratory care immediately prior to the proning session had completed critical care competencies. Further, competencies were associated with performing more SBTs, but not the management of Pplat. The stacked probability Figure 1b from the current study shows how completing competencies impacted the positive discharge status in fewer hospital days. Model 1 demonstrated that both advanced degrees and competencies facilitated a quality discharge to home when measured independently, with competencies having a slightly higher impact. Further, Model 2 showed that high exposure to RTs with competencies increased the frequency of alive discharges by twice when considering ventilator and ICU days.
Findings from this study provide the first empirical evidence that both RTs with baccalaureate or higher education and clinical competencies may improve the outcomes of patients with COVID-19 pneumonia. If >85% of the care being delivered by therapists with advanced degrees were supported in future studies, it could have implications for department hiring practices and entry-level education. Presently, 44% of RTs in the United States have a baccalaureate degree or higher, and only 13.2% of the total number of graduates of entry-level respiratory care programs earned baccalaureate degrees in 2020.46 For respiratory care departments to hire enough RTs with a minimum of a baccalaureate degree, more entry-level baccalaureate programs are needed. Accreditation agencies will need further studies substantiating these findings before changing the entry-level respiratory care degree standards.
The major limitation of this retrospective study is that it does not prove causality. However, the study findings are useful in generating hypotheses for future research to investigate the impact of RT education on patient outcomes. This single-center study was conducted in a clinical department with many (70.8%) RTs with advanced degrees. As a result of a staffing shortage during the surge of the COVID-19 pandemic, the department hired several temporary RTs and students (within one semester of graduating with a master’s degree) who received a short orientation before providing care to critically ill patients. This center utilized a lung protective ventilation protocol which may not be present in all respiratory care departments. Also, due to a shortage of sedatives, RTs were limited in keeping tidal volume in the lung protective range; therefore, exhaled tidal volume data was not addressed in this manuscript. Adherence to PEEP/FiO2 tables was not recorded, thus limiting the ability to further understand the mechanism of RT-driven improved outcomes. Some errors may have occurred with manually inputed SOFA scores. Furthermore, we did not collect patient-level data on the use of inhaled vasodilators which may have also impacted findings. Additionally, we did not collect data on the RT experience in managing ARDS patients, RT to ventilator ratio, and nursing or physician or pharmacist characteristics, which may have influenced the results. As stated earlier, the impact of a single discipline on patient outcomes is not easily discerned.
Conclusion
Respiratory therapist education was associated with improved discharge outcomes for patients with COVID-19 pneumonia. Specifically, the subjects’ discharge quality improved when they received >85% of care from RTs with an advanced degree or who completed annual adult critical care competencies. These preliminary findings suggest that the RT workforce may need advanced education and competency training to provide high-quality, evidence-based care. However, researchers should design robust studies across multiple centers to assess causality and corroborate these findings.
Acknowledgements
We sincerely thank our colleagues at the Rush University Medical Center for their clinical services. We thank Maliha Syed and Aashna Modi for assisting with data collection. We also thank J. Brady Scott for reviewing this manuscript.
Competing interests
The authors have no conflicts of interest to declare.
Funding
This work was supported by the Vision Grant from the American Association for Respiratory Care. The sponsor was not involved in study design, data collection/analysis or manuscript preparation and final submission. All authors had the final decision to submit the manuscript.
Contributors
RK and EB are responsible for all content of the manuscript. RK and EB conceived the idea. RK, AG and EB implemented the study. RK, EB and RM conducted data analysis and interpreted the data. RK, EB, AG and RM drafted the manuscript, all authors reviewed the manuscript for important intellectual content and approved the final manuscript.
Ethical statement
The study protocol was approved by the local institutional review board (ORA#20063001). For analysis, we used datasets which were properly anonymized.
AI statement
The authors confirm no generative AI or AI-assisted technology was used to generate content.