Introduction
The influence of vitamin deficiency on the clinical course and outcomes of acute and chronic internal diseases remains debatable. While knowledge gaps and controversy exist regarding the potential extra-skeletal effects of vitamin D, there is a broad consensus that the high worldwide prevalence of vitamin D deficiency is of concern and requires actions to improve this situation.1 Vitamin D receptors regulate the expression of numerous genes involved in calcium/phosphate homeostasis, cellular proliferation and differentiation, and immune response, and more than 50 targets have been identified involving a broad realm of vitamin D functions.2
In clinical practice, the level of vitamin D is usually assessed by determining the concentration of 25-hydroxyvitamin D since it is characterized by a long half-life and expresses the rate of accumulation of both endogenous and exogenous levels of vitamin D. Vitamin D deficiency is defined as a serum 25-hydroxyvitamin D (25(OH)D) level of <50 nmol/L (<20 ng/mL). In contrast, vitamin D insufficiency is regarded as a 25(OH)D level between 52-72 nmol/L (21-29 ng /mL).3 Vitamin D deficiency may be an underdiagnosed medical condition for years because patients do not typically present with overt clinical signs and symptoms.
At the onset of the pandemic, several studies have reported that serum vitamin D deficiency is associated with an increased risk of worse clinical outcomes of COVID-19 and in-hospital death.4,5 A meta-analysis of eleven cohort studies with 536,105 patients and two randomized clinical trials (RCTs) found that Vitamin D deficiency (< 20 ng/ml) or insufficiency (< 30 ng/ml) was not associated with a significantly increased risk of COVID-19 infection or in-hospital death. The overall quality of evidence (GRADE) for COVID-19 infection and associated death was very low.6 Therefore, the impact of vitamin D on COVID-19 clinical outcomes remains controversial. Prescription of vitamin D supplements in Ukraine, especially at the beginning of the outbreak, was an often-used treatment approach. However, no relevant peer-reviewed published evidence was identified regarding the association between vitamin D levels and the severity of symptoms or mortality due to COVID-19 in Ukraine.
Materials and Methods
This was a single-centred observational cohort study. Inclusion criteria included patients aged ≥ 18 years who were admitted to the hospital with PCR-confirmed COVID-19 and availability of laboratory data (C-reactive protein (CRP), serum 25(OH)D, ferritin). The exclusion criteria were pregnancy, breastfeeding, initial admission to another hospital with the diagnosis of COVID-19, length of hospital stay <24 hours, and transfer to another department/hospital. Seventy-three patients admitted and discharged in 2021 in a specialized department of a private medical centre in Kyiv, Ukraine, due to acute COVID-19 were assessed for eligibility. After a primary assessment, three patients were excluded due to length of hospital stay <24 hours, initial admission in another hospital with a current diagnosis, and transportation to a highly specialized department for acute stroke treatment (see Figure 1).

Demographic and laboratory data (including C-reactive protein (CRP), serum 25(OH)D, ferritin), as well as computed tomography (CT-scan) of the chest, were available from patient electronic records. Blood samples for laboratory tests mentioned above were obtained from all patients at the time of their hospital admission as part of routine blood collection. Serum CRP, ferritin, and 25(OH)D levels were measured by chemiluminescent immunoassay. Diagnosis of SARS-CoV-2 infection was confirmed by a reverse transcription polymerase chain reaction test on a nasopharyngeal swab.
Clinical data, which we used for analysis, included the presence of comorbidities and their nosology; the need for respiratory support; and the severity of COVID-19, defined as mild, moderate, severe, and critical according to World Health Organization criteria. These criteria are based on symptoms at the admission (such as fever, cough, dyspnoea, etc.), respiratory rate, SpO2 measured by a pulse oximeter, signs of lung involvement on CT-scan, the partial pressure of oxygen in the arterial blood (PaO2), and PaO2/FiO2 ratio.7
In-hospital mortality cases were also recorded. Patients included in this study received standardized treatment according to the national protocol for COVID-19 management.8 All patients and/or their representatives provided informed consent. The data were properly anonymized for analysis, and informed consent was obtained at the time of the original data collection. It was a retrospective analysis, and no interventions were performed. In such cases, ethical review is not required in Ukraine.
Statistical Analysis
We expressed continuous variables as mean values ± standard deviations or median values with 25th and 75th quartiles (Q1 and Q3), depending on whether they followed a normal distribution. Categorical variables were presented as the number of cases and percentages. To find differences between continuous data, we used an independent samples t-test. If data did not follow a normal distribution, the Mann-Whitney U test was used for independent samples. We used the Pearson correlation coefficient and performed log transformation for non-normally distributed data to assess the correlation between continuous variables. We used the chi-square test to compare categorical data. Binary logistic regression analysis was conducted to measure crude and adjusted odds ratios (OR). Patients were grouped into two categories based on serum 25(OH)D levels: patients with low vitamin D levels (25(OH)D <30 ng/ml) and patients with adequate vitamin D levels (25(OH)D ≥ 30 ng/ml). The Endocrine Society defines serum 25(OH)D levels <20 ng/ml as deficiency and 21–29 ng/ml as insufficiency.9 Participants requiring conventional oxygen therapy (i.e., nasal cannula or face mask oxygen), continuous positive airway pressure (CPAP), non-invasive ventilation (NIV), or invasive mechanical ventilation (IMV) were considered as patients with respiratory support needs. No patient required Extra Corporeal Membrane Oxygenation (ECMO).
Simple and multivariate binary logistic regression models were considered to identify variables associated with outcomes (mortality, respiratory support need). We presented associations between risk factors and outcomes as odds ratios (OR) with 95% confidence intervals (CI). We considered p-values < 0.05 to be statistically significant. Data were analyzed using MedCalc® Statistical Software version 20.215.10
Results
We included 70 participants for data analysis (three were excluded due to length of hospital stay <24 hours, initial admission in another hospital with current diagnosis and transportation to high specialized department for acute stroke treatment). The median age was 62 years [Q1, Q3: 58; 66.67], with 57.14% female patients. The median follow-up time was eight (5-12) days; six patients (8.57%) died during the study period. Table 1 summarizes participants’ main demographic and clinical characteristics according to serum vitamin D status.
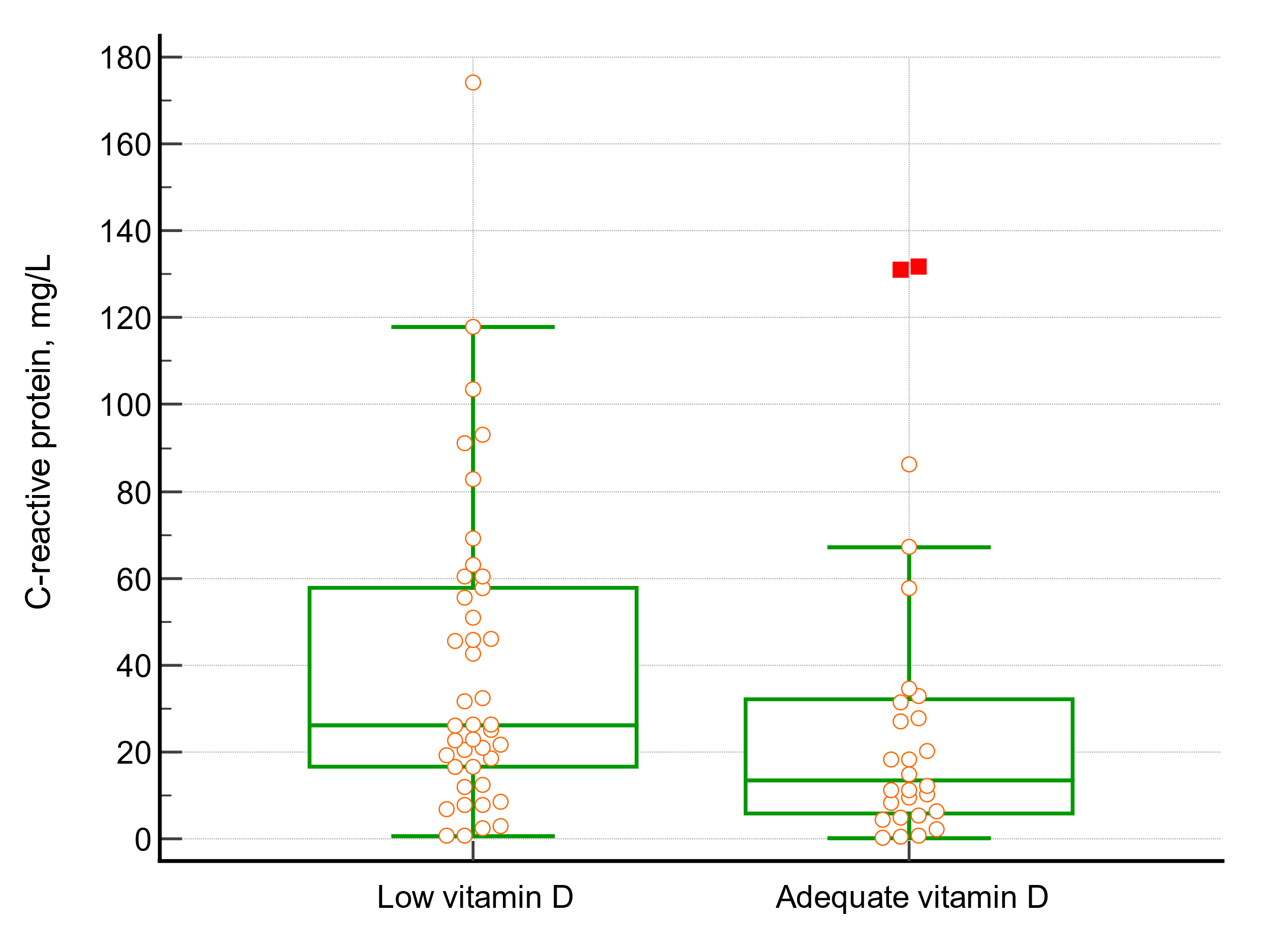
The mean age differs significantly between the group with low vitamin D level (66.48 ± 11.87) and the group with adequate vitamin D level (52.12 ± 14.26,p< 0.0001), but it could be explained by a negative association between vitamin D level and age (Pearson correlation, log-transformed data: r= -0.3770 p=0.0013). The level of CRP differs in the group with 25(OH)D <30 ng/ml [median 26.14, Q1, Q3: 16.61; 57.79] and in the group with 25(OH)D levels ≥30 ng/ml [median 13.43, Q1, Q3: 8.84; 27.58], p= 0.044. Figure 2 shows the difference in inflammatory marker CRP between patients with 25(OH)D levels <30 ng/ml and those with 25(OH)D levels ≥30 ng/ml.
d_levels___30_ng_ml_(low.png)
Meanwhile, patients with comorbidities had lower serum vitamin D levels (27.1 ± 11.66) than patients without comorbid diseases (34.32 ± 11.99), p=0.0177.
Results suggested that inadequate vitamin 25(OH)D was associated with an increased risk of respiratory support need (OR 2.925; 95% CI 1.0839 to 7.8931). However, after adjustment for age, gender (Model 1) and for age, gender, and comorbidities (Model 2) OR was lower than crude OR and not statistically significant. Table 2 includes a brief summary of predictors of respiratory support therapy need using binary logistic regression analysis.
The length of stay did not differ between the group with low vitamin D levels [median 9, Q1, Q3: 6, 14] and with adequate vitamin D levels [median 7, Q1, Q3: 4, 11.5], p= 0.0695.
Vitamin D serum levels did not significantly differ in patients who died during hospitalization compared to those who survived. Using binary logistic regression analysis, we found that vitamin D status did not predict mortality (OR 3.65; 95% CI 0.40 to 33.05).
Discussion
The results of this study indicate a significant difference in mean age between the group with low vitamin D levels and the group with adequate vitamin D levels. However, this difference can be explained by the negative correlation between vitamin D levels and age. This finding is consistent with previous research suggesting that vitamin D levels tend to decline with age.11,12
CRP has been recognized as an important factor to consider in patients with COVID-19. Elevated CRP levels are a common laboratory finding in patients with COVID-19 and have been associated with disease severity and poor clinical outcomes, including higher mortality rates.13 Therefore, our finding that patients with low vitamin D levels have higher levels of CRP may have diagnostic and prognostic value in the management of COVID-19. Furthermore, the link between low vitamin D levels and elevated CRP levels may suggest potential therapeutic targets for the treatment of COVID-19. Other studies have yielded similar results. The investigation carried out by Italian scientists explored the potential connection between vitamin D levels and the inflammatory response in COVID-19 patients. Their study focused on 93 individuals with COVID-19-induced pneumonia showing that patients with low levels of vitamin D (defined as 25(OH)D ≤ 20 ng/ml) had significantly higher CRP levels than those with 25(OH)D > 20 ng/ml.14 In another study by Demir et al. conducted in Turkey among COVID-19-positive patients, the group with vitamin D levels of >30 ng/ml had significantly lower CRP levels than other groups where vitamin D level was less than 30 ng/ml (mean 0.39 ± 0.16 in group IV with 25(OH)D > 30 ng/ml vs mean 10.99 ± 4.10 in group III with 25(OH)D 20–30 ng/ml vs mean 20.14 ± 4.55 in group II with 25(OH)D 10–20 ng/ml vs mean 22.49 ± 2.88 in group II with 25(OH)D less than 10 ng/ml).15
We found that inadequate vitamin 25(OH)D was associated with an increased risk of respiratory support need (OR 2.925; 95% CI 1.0839 to 7.8931). However, after adjustment for age, sex, and comorbidities, we could not confirm this association. Some studies also researched possible links between the need for respiratory support and vitamin D level. Similarly to our study, Adami et al. also did not find a difference in the types of respiratory support needed (oxygen therapy delivered by nasal cannula, masks, non-invasive and invasive mechanical ventilation) in hospitalized COVID-19 patients with vitamin D deficiency vs. patients with serum 25(OH)D ≥20 ng/ml. However, they concluded that patients with hypoxemia (defined as pO2 <60 mmHg) had significantly lower levels of serum vitamin D level compared to patients with pO2 ≥60 mmHg (13.3 ng/mL vs 20.4 ng/mL respectively, p=0.03).16
The association between vitamin D levels and the length of stay in the hospital remains debatable. We did not find a difference in hospital stay duration between the group with low vitamin D levels and the group with adequate vitamin D levels. The same result was reported by Adami et al.16
Reis et al. mentioned in their study that in patients hospitalized with moderate-to-severe COVID-19, individuals with severe 25(OH)D deficiency (<10 ng/mL) showed a tendency towards an extended duration of hospitalization when compared to patients with higher 25(OH)D concentrations. However, this relationship was not significant in the multivariate Cox regression model.17
We consider that in Ukraine, elderly patients with comorbidities and low serum vitamin D levels (25(OH)D <30 ng/ml) hospitalized due to COVID-19 should receive increased attention, as these factors may lead to worse outcomes. We did not find similar studies conducted on Ukrainian adults; therefore, we could not compare our results for this population.
Despite findings from some previous studies that indicate a relationship between serum 25(OH)D levels and the severity of COVID-19 infection,14,18,19 our results suggest that low vitamin D levels cannot be used as a sole factor for predicting negative outcomes such as respiratory support need and mortality. We believe that many factors, such as age, comorbidities, and disease severity, could confound the relationship between vitamin D levels and COVID-19 outcomes. However, we think measuring vitamin D levels in hospitalized COVID-19 patients could be one of several factors that may help doctors make clinical decisions.
Limitations
Our study has a few limitations. Generalizing the study’s results to a wider population may be challenging due to the study’s reliance on data from only one centre and sample size. In addition, the research was conducted in a private medical centre; therefore, it may be prone to selection bias, as patients who seek care at such centres may have different demographic, socioeconomic, or health-related characteristics than those who receive care in public hospitals.
Conclusion
Although the role of vitamin D as solely factor of mortality and respiratory support need appears overestimated, the differences in the level of inflammatory marker CRP between patients with adequate vitamin D and low vitamin D status suggest that vitamin D level needs to be considered in hospitalized patients with COVID-19, especially in elderly patients with comorbidities.
Acknowledgements
We sincerely thank our colleagues in the laboratory department of Medical Centre Universal Clinic “Oberig” for carrying out the necessary laboratory tests and to doctors and nurses for their dedicated work during the COVID-19 pandemic.
Competing interests
The authors have no conflicts of interest to declare.
Funding
This study did not receive any specific grant from public, commercial or not-for-profit funding agencies.
Contributors
The authors confirm their contribution to the paper: study conception and design: [VB]. Data collection, analysis and interpretation of results: [SS]. Draft manuscript preparation: [VB], [SS]. All authors reviewed the results and approved the final version of the manuscript.
Ethical statement
All patients and/or their representatives gave informed consent. For analysis, we used datasets which were properly anonymized.
AI statement
The authors confirm no generative AI or AI-assisted technology was used to generate content.