Introduction
Respiratory therapists (RTs) are healthcare professionals with specialized expertise in cardiopulmonary health.1,2 Their clinical decision-making is expected to be evidence-based, integrating clinical experience, the best available research evidence, and patient perspectives to ensure high-quality care.3,4 Because respiratory care frequently requires rapid decision-making, coordination with multiple disciplines, and adaptation to complex clinical contexts, RT practice is inherently interprofessional in nature.3–5 RTs are often integral members of interprofessional teams both within and outside hospital settings, working alongside physicians, nurses, and other healthcare professionals.3–5
In the United States, approximately five million patients are admitted to intensive care units (ICUs) annually.6 Owing to medical advances over the past decades, millions of these patients now survive to discharge.6 One of the key reasons for this improved survival is the care delivered by multidisciplinary teams, including physicians, nurses, advanced practice providers, RTs, dietitians, physical therapists, case managers, and others—who collaborate to achieve optimal outcomes.7 In ICU settings, where patients often require mechanical ventilation, airway management, oxygen therapy, and continuous cardiopulmonary monitoring, RTs contribute essential expertise to team-based decision-making.1,2 In today’s cost-conscious healthcare environment, the efficiency of care delivery across institutions is under increasing scrutiny.8 The cost-effectiveness of RTs continues to require evaluation in many countries.8,9 In healthcare systems without specialized RTs, full-time nurses are often responsible for ICU mechanical ventilation, necessitating additional training and recruitment.8,9 However, many ICU staff may not receive adequate professional education and training in ventilator management.8,9 Without sufficient staffing and specialized training, delivering satisfactory respiratory care remains a challenge.8 These workforce and training challenges further underscore the importance of structured interprofessional education that prepares healthcare professionals to understand RT roles, collaborate effectively in respiratory care, and optimize team performance in high-acuity environments.
Interprofessional practice (IP) constitutes a critical component of healthcare delivery.10,11 Collaborative team-based care improves provider morale, reduces communication barriers, enhances mutual understanding between disciplines, strengthens professional confidence, and facilitates both intra- and interprofessional communication.10,11 More importantly, patients benefit directly when healthcare professionals work together to ensure continuity of care and patient safety.12,13 Interprofessional education (IPE), commonly understood as occasions when learners from two or more professions learn with, from, and about each other, provides an educational foundation for developing these collaborative competencies.10,11 Within this context, RTs are well positioned to serve as advanced providers in multidisciplinary teams. The RT profession has increasingly sought to expand its role across the continuum of care, including prevention and health promotion, emergency care, outpatient services, and physician office practice.14 The American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR) has issued clinical competency guidelines recommending that RTs be included among the providers delivering comprehensive pulmonary and critical care rehabilitation services.15 As key members of multidisciplinary teams, RTs contribute holistic treatment strategies for patients with pulmonary diseases throughout the healthcare continuum.3–5,16 During the COVID-19 pandemic, the global healthcare industry recognized the crucial role and significance of RTs in providing respiratory care.17–20 In healthcare, effective teamwork depends on shared goals, role clarity, interdependence, and collective responsibility among professionals from different disciplines.21–24 The World Health Organization has identified interprofessional collaboration as an essential strategy to address the complex challenges of the global health workforce.25,26 In respiratory and critical care settings, such collaboration is particularly important because poor teamwork and communication are associated with patient harm, adverse events, and preventable medical errors.27–29 Therefore, structured interprofessional education is needed to prepare healthcare professionals to communicate effectively, understand one another’s roles, and deliver safer patient-centered care. In today’s complex healthcare environment, providers must acquire fundamental collaborative skills to ensure patient safety and improve care outcomes.30,31 More than a decade ago, the Institute of Medicine (IOM) emphasized in its report that practice, education, and policy recommendations should promote collaboration, integrating interprofessional education (IPE) into curricula and clinical practice. Nearly ten years later, nursing programs continue striving to overcome barriers to IPE implementation in order to prepare a competent workforce.32 IPE brings together students and practitioners from different disciplines, creating an environment in which participants learn to appreciate each other’s unique expertise.33 The core competencies developed through IPE include communication, teamwork, role clarification, values, and ethics.34 These competencies are critical for improving patient care, as they ensure seamless collaboration among providers and the formulation of comprehensive, patient-centered treatment plans, thereby enhancing both care quality and patient safety.33,35
Therefore, examining the role of RTs in interprofessional practice (IP) and interprofessional education (IPE) represents a critical area of inquiry. However, despite the recognized importance of RTs in team-based respiratory care, their representation in IPE curricula, educational research, and interprofessional outcome assessment remains less clearly characterized than that of other health professions. Accordingly, this narrative review sought to examine how RTs have been incorporated into IP and IPE initiatives, summarize the educational and clinical outcomes reported, and identify current knowledge gaps to guide future research and educational development. Specifically, this review addressed the following research questions: (1) How have respiratory therapists been incorporated into interprofessional practice and interprofessional education initiatives? (2) What educational and clinical outcomes have been reported? and (3) What knowledge gaps remain to guide future research and educational development?
Methods
Review design and framework
The study group conducted this narrative review following Ferrari’s narrative review framework, which provides guidance for structuring, synthesizing, and reporting literature reviews in a narrative style.36 The framework was used to guide a focused and transparent synthesis of literature on IP and IPE involving RTs and respiratory therapy students. The review was organized around three domains: implementation models, educational and practice-related outcomes, and remaining knowledge gaps.
Search strategy
A search was conducted in PubMed, ERIC, and ProQuest from database inception to September 2025. The search strategy combined controlled vocabulary and free-text terms related to respiratory therapy and interprofessional education, including “respiratory therapist,” “respiratory therapy student,” “respiratory care,” “interprofessional education,” “interprofessional learning,” “team-based learning,” “multidisciplinary,” and “collaborative practice.” Search strategies were adapted for each database. Reference lists of eligible studies and relevant reviews were also manually screened to identify additional records.
In addition to the database searches, Google Scholar was used to identify relevant grey literature and supplementary sources. Searches combined terms related to respiratory therapy and interprofessional education, including “respiratory therapist,” “respiratory therapy student,” “respiratory care,” “interprofessional education,” “interprofessional learning,” “team-based learning,” “multidisciplinary care,” and “collaborative practice.” The first several pages of results were screened for relevance, with particular attention to reports, educational guidelines, policy documents, consensus statements, and scholarly materials not captured in PubMed, ERIC, or ProQuest. Reference lists of relevant grey literature sources were also manually reviewed. Grey literature was included when it provided substantive information on educational models, implementation strategies, interprofessional competencies, or clinical and educational outcomes related to respiratory therapist involvement in interprofessional education.
Eligibility criteria
Peer-reviewed English-language studies were eligible for inclusion if they examined RTs or respiratory therapy students and reported on IPE, interprofessional learning, collaborative practice, or team-based learning activities in healthcare or health professions education contexts. Studies were excluded if they focused exclusively on simulation-based technical training without an interprofessional component, did not include RTs or respiratory therapy students, were conference abstracts, commentaries, editorials, or were published in languages other than English.
Study selection
Titles and abstracts were screened to identify potentially relevant records. Full texts of eligible or potentially eligible articles were subsequently reviewed. Studies were selected based on their relevance to RTs, RT students, IPE, interprofessional learning, collaborative practice, and team-based healthcare delivery. Because this study was conducted as a narrative review rather than a systematic review or meta-analysis, formal risk-of-bias assessment, methodological quality scoring, and quantitative synthesis were not performed. Instead, the literature was narratively synthesized to identify implementation models, reported educational and clinical outcomes, and existing research gaps related to respiratory therapist–inclusive IPE.
Data extraction
Data were extracted using a standardized form that captured bibliographic details, study design, country or region, study period, educational or clinical setting, participant characteristics, health professions represented, sample size, intervention or learning activity, comparator details when available, reported outcomes, and methodological information relevant to interpretation. Data extraction was conducted independently by two reviewers and reconciled through discussion. Because of heterogeneity in study designs, settings, participants, interventions, and outcome measures, findings were synthesized narratively rather than statistically. The synthesis was organized around implementation models of RT-inclusive IPE, reported educational and practice-related outcomes, and knowledge gaps in the existing literature.
Results
Study selection and characteristics of included studies
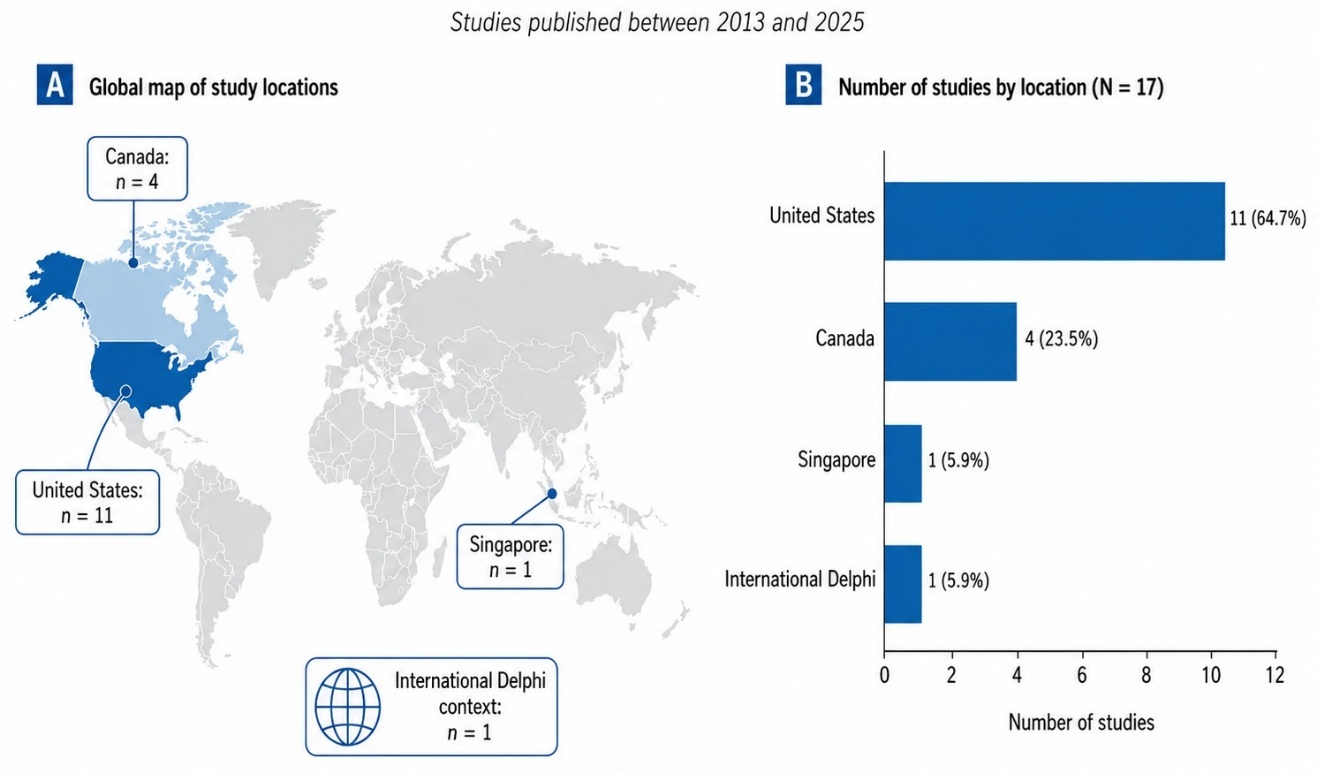
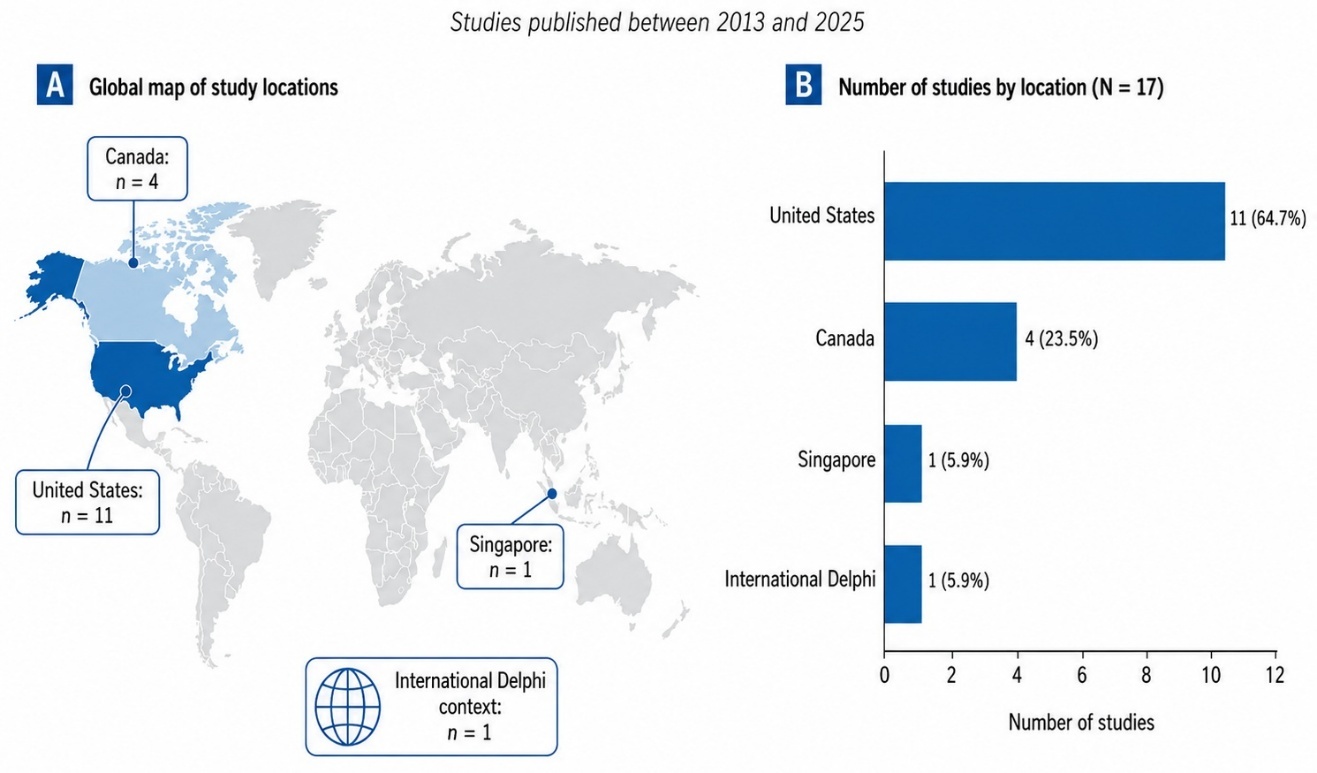
A total of 17 studies met the inclusion criteria. Included records comprised empirical studies as well as selected protocol, Delphi, and commentary reports that addressed RT involvement in IPE. These were conducted between 2013 and 2025 across the United States (n = 11),5,14,21,33,37–43 Canada (n = 4),35,44–46 Singapore (n = 1),26 and an international Delphi context (n = 1)47 The study selection process and geographic distribution of the included records are shown in Figure 1, and the summary characteristics of the included records are presented in Table 1. Cross-sectional surveys were subject to non-response and selection bias.5,39,42 Delphi, commentary, and protocol-based reports had inherent methodological constraints, while exploratory studies were limited by small sample sizes and generalizability.14,26,37,44,47
Implementation of IPE activities involving RTs
IPE activities involving RTs were most often delivered through simulation-based interventions (n = 9),21,33,35,38,40,41,43,45,46 including standardized patients, interprofessional scenarios, and TeamSTEPPS-based training. Workshops or seminars were reported in 3 studies,33,35,41 and team competence training was noted in 2 studies.45,46 In clinical contexts, RTs were integrated into NICU rounds,37 primary care teams,44 and ICU recovery clinics.14 One Delphi study underscored the underrepresentation of RTs in international IPE research agendas.47 The characteristics of the included studies and their corresponding settings are summarized in Table 2.
Outcomes assessed and evaluation approaches
Outcomes commonly assessed included collaborative competencies, teamwork confidence, interprofessional communication, knowledge of mechanical ventilation, and faculty perceptions of IPE.5,14,21,26,33,35,37–47 The intervention focus, outcomes assessed, and key findings of the included studies are summarized in Table 3. No single standardized instrument was applied across studies; instead, evaluations ranged from validated team competence scales to faculty surveys and custom-designed metrics.
Reported educational effects of RT-inclusive IPE interventions
Across intervention-based studies, RT-inclusive IPE was generally associated with positive educational outcomes, particularly in collaborative competencies, teamwork confidence, communication, and role recognition. Simulation-based interventions enhanced collaborative competencies, teamwork confidence, and communication skills.33,35,41,43 Curricular integration improved knowledge of mechanical ventilation and strengthened role recognition of RTs.21 Faculty surveys highlighted generally supportive attitudes toward IPE, though challenges included limited institutional exposure and discrepancies in competency prioritization.5,39 Notably, RT faculty emphasized communication as the most critical competency, while ethics was rated lower compared with other health professions.42
Discussion
The evolving role of respiratory therapists in interprofessional practice
This narrative review highlights that RT-inclusive IP and IPE initiatives occupy an important but still underexamined role within health professions education. Across the included literature, RT participation was most often discussed in relation to team-based learning, simulation-based education, role clarification, and collaborative clinical practice. Overall, RT participation in IPE has been shown to enhance teamwork, clarify professional roles, and improve clinical knowledge, particularly when implemented through simulation-based education.5,21,33,35,38–43,45–47 Clinical studies have also demonstrated the contributions of RTs in neonatal care, primary care integration, and ICU recovery settings.14,26,37,44,47
Historically, the professional prominence of RTs has been rooted in hospital practice, particularly within critical care.44 While this remains true today, the scope of RT practice continues to expand.44 The broad range of clinical responsibilities and the depth of cardiopulmonary expertise possessed by RTs suggest that they can provide valuable background knowledge and insights across various health science disciplines.47 In recent years, however, the role of RTs has increasingly extended into community settings, including asthma and COPD clinics, pulmonary rehabilitation centers, and community health facilities.44 Following the COVID-19 pandemic, hospitals worldwide are facing an increasing burden of post-intensive care syndrome (PICS).14 Moreover, health systems that were already under strain due to factors such as increasing clinical complexity, rising healthcare costs, rapid technological advancement, and growing patient expectations now face even greater pressure for innovation and collaboration.43,44 The trend toward multidisciplinary teams providing primary healthcare (PHC) has emerged as an effective model.48,49
As cardiopulmonary experts, RTs have been recognized by AACVPR, whose clinical competency guidelines recommend that RTs be included among providers of comprehensive pulmonary and critical care rehabilitation services.15 Within such teams, RTs serve as key members who deliver integrated therapeutic strategies and optimize outcomes for patients with pulmonary disease across the continuum of care.14 Presently, RTs collaborate within multidisciplinary teams to integrate disease prevention and health promotion into care systems—rather than intervening only when patients reach critical illness, as was often the case in the past.44 In their professional practice, RTs base clinical decision-making on evidence, combining clinical experience, the best available data, and patient perspectives to ensure high-quality care.3,4 At the same time, they must understand and actively engage with emerging research that may shape their practice.3 RTs’ specialized knowledge and skills should guide how respiratory care is practiced and influence how research is conducted, especially when empirical findings directly affect the way RTs deliver patient care.50,51 This expanding scope makes RTs particularly relevant to IPE because respiratory care often requires real-time coordination among multiple professionals, including physicians, nurses, rehabilitation specialists, pharmacists, dietitians, and discharge planning teams. Therefore, RT-inclusive IPE should not be viewed solely as an educational requirement, but as a preparation for the collaborative realities of respiratory care delivery.
Underrepresentation of RT perspectives in research and education
However, a concerning reality is that much of the evidence informing respiratory care has not included the perspective of RTs.47 Several authors have also identified distinct knowledge gaps, both practical and theoretical, that are unique to the RT profession.52,53 For example, studies focusing on mechanical ventilation management or high-flow nasal cannula therapy often did not include RTs in expert panels.54–58 Even when RTs were included, their representation was minimal.59–62 This repeatedly underscores that the expert role of RTs in evidence-based respiratory care remains insufficiently defined.47 The limited inclusion of RT perspectives has implications beyond research representation. It may also shape how respiratory care competencies are taught, how interprofessional learning objectives are constructed, and how outcomes relevant to RT practice are measured. Without sufficient RT input, IPE curricula may emphasize generic teamwork skills while overlooking profession-specific contributions such as ventilator management, airway decision-making, oxygen therapy optimization, and pulmonary rehabilitation planning. Consequently, research in respiratory therapy conducted by other health disciplines may not fully capture the specific knowledge boundaries or practical constraints unique to RTs.50,51 It is well recognized that siloed practice undermines institutional efforts to deliver comprehensive health and wellness services.63,64 A key Delphi study emphasized that RTs must employ critical thinking and make clinical decisions grounded in the best current evidence while integrating patient values and clinical experience.47 Therefore, RTs must also contribute to the development of their own professional practice. They should be encouraged to engage in future research to ensure that emerging empirical evidence includes their perspectives. Enhancing the representation of RTs in research is essential and may require dedicated education, mentorship, and the removal of barriers that currently limit their participation.47,51
Educational value of RT-inclusive IPE
To eliminate these barriers, RT educators must ensure that advanced curricula and training programs address the expanding roles of RTs as experts across diverse healthcare environments.14 This will better prepare future RTs to serve as primary providers within multidisciplinary rehabilitation teams.14 Collaborative case management with other professionals, such as physicians, nurses, social workers, dietitians, and physical or occupational therapists, can deliver the most comprehensive care, particularly in respiratory medicine.44 Evidence shows that formal opportunities for shared decision-making and structured communication forums among healthcare professionals are mutually beneficial.65,66 Effective collaboration enhances staff satisfaction and patient outcomes through shared management decisions.65,66 Similarly, when RTs actively participate in ward rounds, communication among interprofessional team members improves, and the timeliness of respiratory care orders increases.37 Changes in perception and attitude toward interprofessional teamwork are considered prerequisites for behavioural change and, ultimately, for improvements in patient safety outcomes.38 Early exposure of healthcare students to multidisciplinary knowledge fosters collaboration, builds interprofessional competencies, and prepares them to deliver patient-centered care after entering professional practice; an essential skill in today’s complex healthcare systems.21,43,67
According to established IPE frameworks, six core IPE competencies include communication, collaboration, conflict resolution, patient-centered care, understanding of roles and responsibilities, and effective team functioning.35,46 IPE further emphasizes four key collaborative practice competencies: developing mutual respect among professionals, understanding professional roles, communicating effectively, and building healthy team relationships.68 Opportunities to cultivate team cohesion are critical for positive interprofessional experiences, and introductory team-building exercises help students better understand one another.21,40
Students often describe IPE experiences as transformative, as they witness its benefits for patient care and embrace challenges and responsibilities within interprofessional teams—particularly in acute care settings where collaborative practice optimizes outcomes.21,69,70 Over recent years, many healthcare accreditation bodies have introduced new curriculum standards requiring IPE participation. The Commission on Accreditation for Respiratory Care explicitly mandates through Standard 4.05 that all entry-to-practice RT programs must include IPE.71 This standard specifies: “Graduates must be able to work in interprofessional teams and communicate effectively with diverse populations. Programs must prepare students to collaborate with individuals of varying ages, abilities, and ethnicities”.71 When team members understand and openly engage in such collaborative models, preventable medical errors can be avoided.38 Although no standardized method for implementing IPE currently exists, simulation-based training (SBT) is one of the most widely used and effective active learning strategies, providing RTs with valuable IPE experience.38,43 Simulation-based IPE (SIM-IPE) has been shown to positively influence students’ attitudes and perceptions of interprofessional collaboration.33,35,38,41,43,45 Regardless of the simulation modality, whether manikins or standardized patients, outcomes remain similarly effective.46 However, simulation-based IPE should not be interpreted as a complete substitute for longitudinal interprofessional learning in authentic clinical environments. Many studies primarily assessed short-term changes in attitudes, perceptions, or self-reported confidence, whereas fewer studies examined sustained behavioural change, transfer of learning to clinical practice, or patient-related outcomes. Future RT-inclusive IPE research should therefore connect simulation-based learning with clinical placement, reflective practice, and longitudinal assessment. Although the available RT literature remains limited, the educational outcomes identified in this review generally align with the broader principles of interprofessional education, emphasizing communication, teamwork, role clarification, and collaborative practice. At the same time, the evidence synthesized in this review indicates that RT-inclusive IPE has been evaluated predominantly through educational outcomes, with relatively few studies examining sustained changes in clinical practice or patient care.
Furthermore, hybrid learning strategies that combine pre-simulation videos, team role discussions, and progressive learning sequences have been shown to enhance learning outcomes.41,45,46 When designing learning objectives, educators should recognize that situational awareness represents an advanced expectation for undergraduate learners, and objectives should specify a novice level of achievement.41,45,46 As students advance through simulation exercises, their growing familiarity with professional roles, along with guided reflection on overlapping responsibilities, encouragingly fosters critical self-evaluation of their actions.35 Thus, students should be provided with reflective tools to analyze their own roles and those of others, thereby strengthening role clarity, particularly within the context of individual practice and team leadership behaviours.35
Barriers to implementation from the educator perspective
At the same time, both faculty and students in healthcare programs express concern about time constraints and the feasibility of incorporating additional IPE content into already dense curricula.39,72,73 Therefore, it is also crucial to consider the perspectives of RT educators. While RT educators widely acknowledge IPE as an essential component of RT education, they also report significant challenges integrating it into existing programs.5 Among IPE competencies, communication is rated as the most important, followed by teamwork and collaboration, understanding of roles and responsibilities, and finally, ethics.5,42 Ethics may have been ranked lower because ethical standards and guidelines are already emphasized in domains outside of IPE.39
Survey research further indicates that for RT faculty, the most common barriers to implementing IPE include faculty attitudes, scheduling and logistics, curricular demands, administrative limitations, and time.39 Faculty resistance often stems from concerns about change and uncertainty regarding IPE’s impact on professional effectiveness.39 Overall, RT educators express apprehension about developing curricula that must meet the requirements of multiple disciplines while coordinating mutually acceptable schedules. Despite these challenges, most faculty remain supportive of incorporating IPE into their curricula, and perceived opportunities and barriers are similar across program types.39 Interestingly, educators with bachelor’s and master’s degrees report greater knowledge and stronger beliefs about IPE compared with those teaching at the associate degree level.5 Ultimately, the success of IPE programs depends on several key factors: administrative support, interprofessional organizational structures, dedicated faculty, and experienced educators.5,74 Accordingly, RT educators hold a positive attitude toward IPE and generally agree on its importance in RT curricula, with most expressing a desire for greater emphasis on IPE integration in the future.5
Future directions for RT-inclusive IPE
Taken together, these findings suggest several priorities for future RT-inclusive IPE. First, RTs and RT educators should be involved from the earliest stages of curriculum design rather than included only as participants in predetermined interprofessional activities. Second, outcome evaluation should incorporate both general IPE competencies and RT-specific indicators, such as respiratory assessment, ventilator-related communication, escalation of respiratory deterioration, and collaborative discharge planning. Third, institutions should develop sustainable IPE structures that address scheduling, faculty development, administrative support, and curricular alignment across disciplines. These steps may help ensure that RT-inclusive IPE is not episodic or symbolic, but integrated into the broader educational mission of preparing collaborative healthcare professionals.
Strengths and Limitations
This review provides one of the first comprehensive syntheses of RT-inclusive IPE across educational and clinical settings. By integrating findings from multiple study designs and healthcare contexts, the review offers a broad overview of current implementation models and educational outcomes. However, several limitations should be acknowledged. First, the available evidence remains limited in quantity and is concentrated primarily in North America. Second, substantial heterogeneity in study design, outcome measures, and educational settings precluded quantitative synthesis. Third, many studies evaluated educational outcomes such as participants’ perceptions, attitudes, confidence, and role awareness using self-reported measures, whereas evidence regarding sustained behavioural change, improvements in interprofessional team functioning in clinical practice, and patient-related outcomes remains limited. Consequently, the findings should be interpreted as descriptive rather than definitive evidence of effectiveness.
Conclusion
This narrative review highlights the important but underdeveloped role of RTs and respiratory therapy students in IP and IPE. Current evidence suggests that RT-inclusive IP and IPE initiatives can enhance teamwork, communication, professional role clarity, collaborative competence, and clinical preparedness across educational and clinical contexts. However, RT perspectives remain insufficiently represented in curriculum design, implementation, research, and outcome evaluation. Future studies should use standardized assessment tools, include longitudinal follow-up, and examine the impact of RT-inclusive IPE on collaborative practice and patient care outcomes. Integrating IPE as a core component of RT education and continuing professional development may strengthen interprofessional collaboration, improve patient safety, and support higher-quality respiratory care.
Availability of Data and Materials
Data sharing is not applicable to this article, as this review did not generate or analyze any new datasets. All information presented is derived from previously published studies cited in the manuscript.
Ethics Approval and Consent to Participate
Ethics approval and consent to participate were not applicable, as this study was a literature review and did not involve human participants, human data, or animal experiments.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure statement
All authors have completed the ICMJE uniform disclosure form and declare no conflict of interest.
AI Statement
The authors confirm no generative AI or AI-assisted technology was used to generate content.