Introduction
Coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and can result in lung impairment.1,2 Infected lung tissue exhibits multiple pathophysiological changes, including diffuse alveolar epithelial injury, capillary damage with hemorrhage, hyaline membrane formation, and pulmonary consolidation.3,4 These changes can impair the pulmonary diffusing capacity for carbon monoxide (DLCO), particularly in individuals recovering from severe or critical infection.5 However, impaired DLCO has also been reported in individuals recovering from mild to moderate COVID-19.6,7 Several clinical factors, including sex, smoking status, dyspnea, and body mass index (BMI), have been reported to be associated with impaired DLCO,6 and comorbidities such as emphysema and pulmonary hypertension may also contribute.8,9 Despite these observations, the mechanisms underlying post-COVID pulmonary function impairment remain incompletely understood. Prolonged systemic inflammation and pulmonary vascular injury have been proposed as potential contributors.10
Reduced DLCO has been widely documented in patients recovering from severe or critical COVID-19. However, most individuals infected with SARS-CoV-2 experience mild to moderate disease, and emerging evidence suggests that impaired DLCO is not uncommon even in these non-severe cases. Furthermore, evidence indicates that pulmonary diffusion abnormalities are not limited to severe COVID-19.11 Nearly one-third of patients with mild disease demonstrate impaired DLCO within approximately one month after diagnosis, and about one-fifth exhibit a restrictive spirometric pattern.7 Increasing age has been shown to significantly elevate the risk of impaired DLCO, with an approximate 10% increase in the odds per additional year of age, while the presence of restrictive lung physiology markedly increases the likelihood of diffusion impairment.7 In contrast, certain upper respiratory symptoms, such as excessive night sweats and nasal congestion, have been associated with a lower probability of impaired gas exchange.7 Furthermore, pooled analyses suggest that severe disease at diagnosis substantially increases the prevalence of DLCO impairment, and the definition used to classify abnormal DLCO (e.g., <80% predicted) may significantly influence reported prevalence estimates.7 Moreover, a previous study found that lung function abnormalities after mild COVID-19 infection were associated with the development of ground-glass opacities rather than lung consolidation.12 Ground-glass opacities are associated with local dysregulations involving markers of endothelial and epithelial injury, suggesting a degree of venous thromboembolism, endothelial dysfunction, and abnormalities in cardiopulmonary circulatory physiology, which may in turn contribute to DLCO impairment.13 Nevertheless, existing studies often focus on specific subgroups or single-centre cohorts, which may limit generalizability.
Despite the growing literature, it remains unclear which clinical variables are statistically associated with impaired DLCO in patients recovering from COVID-19, particularly in multicentre populations with varying disease severities. Clarifying these associations may help inform risk stratification and follow-up planning in post-COVID care. Therefore, the present study aimed to identify clinical variables associated with impaired pulmonary diffusing capacity in patients recovering from COVID-19 using a secondary analysis of multicentre datasets. We hypothesized that demographic characteristics and pulmonary function parameters would be associated with reduced DLCO following recovery from COVID-19.
Materials and methods
Study design
This study was conducted as a secondary analysis of multicentre datasets, including adults with laboratory-confirmed COVID-19 who underwent standardized pulmonary function testing during the post-acute recovery phase. The original datasets were collected prospectively across multiple centres and included individuals spanning a spectrum of initial disease severities (mild to critical).14 The present analysis specifically aimed to identify independent clinical variables associated with impaired pulmonary diffusing capacity following recovery from COVID-19.
Participants
Eligible participants were adults (≥18 years) with a prior confirmed SARS-CoV-2 infection who completed pulmonary function testing at follow-up.14 Participants were excluded if they had any of the following physiologically implausible results: forced vital capacity (FVC) ≥ total lung capacity (TLC); alveolar volume (VA5S) ≥ TLC by ≥ 0.20 L; forced expiratory volume in one second (FEV1)/FVC ratio ≥ 0.9.14 For the present secondary analysis, 572 post-COVID-19 patients with complete pulmonary function data and relevant clinical variables were included.14 The source multicentre dataset also included 76 healthy controls; however, these individuals were not part of the target population for the present secondary analysis and were therefore included. In addition, post-COVID participants with missing DLCO measurements or incomplete key covariate data were excluded from the complete-case analysis. Only patients classified as post-COVID-19 were included in the present study.
Procedure
Pulmonary function testing
Pulmonary function tests were obtained from multicenre datasets in which testing was performed at each participating center according to international standards (ATS/ERS guidelines) during the post-acute recovery phase; however, detailed information on the exact timing of follow-up assessments, site-specific quality control procedures, and hemoglobin correction was not consistently available across all datasets.15–24 Measurements included FVC, FEV1, the FEV1/FVC ratio, TLC, and the diffusing capacity of the lung for carbon monoxide (DLCO).25 Spirometry was used to measure FVC, FEV1, and FEV1/FVC ratio to detect obstructive patterns. Whole-body plethysmography was used to measure TLC to identify restrictive lung impairments.14 DLCO was assessed using standardized single-breath techniques according to international guidelines.25 Impaired DLCO was defined as a DLCO z-score < -1.645 below the lower limit of normal (LLN) based on the Global Lung Function Initiative (GLI) reference equations.25
Clinical and pulmonary variables
Demographic and clinical variables were extracted from the original multicentre datasets, including age, sex, and body mass index (BMI). Pulmonary function parameters obtained during follow-up assessment included FVC, FEV1, the FEV1/FVC ratio, TLC, and DLCO.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki. As a secondary analysis of de-identified multicentre datasets, no additional patient contact occurred. Ethical approval and informed consent were obtained in the original studies from which the datasets were derived.14
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics, version 26. Continuous variables were tested for normality using the Shapiro-Wilk test. Normally distributed variables were expressed as mean ± standard deviation (SD), whereas non-normally distributed variables were presented as median (interquartile range). Categorical variables were summarized as frequencies and percentages. Between-group comparisons (impaired vs. non-impaired DLCO) were performed to describe baseline differences using an independent t-test or Mann-Whitney U test for continuous variables, and a chi-square test or Fisher’s exact test for categorical variables. Univariable logistic regression was used as an initial screening step to identify variables potentially associated with impaired DLCO. Variables with p < 0.10 in univariable analysis, together with clinically relevant variables, were considered for inclusion in the multivariable logistic regression model. Candidate variables considered for model inclusion included age, sex, body mass index (BMI), forced vital capacity (FVC), forced expiratory volume in one second (FEV1), and total lung capacity (TLC), based on prior literature and clinical relevance. Given the exploratory nature of this secondary analysis, the final model was intended to identify statistical associations rather than establish a stable clinical prediction model. Multicollinearity was assessed using variance inflation factors (VIF). Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were reported. Model calibration was evaluated using the Hosmer-Lemeshow goodness-of-fit test; however, no graphical calibration assessment was performed. Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC), representing apparent performance in the development dataset. A two-sided p-value < 0.05 was considered statistically significant.
Results
The baseline characteristics of post-COVID-19 patients are presented in Table 1. This secondary analysis included only post-COVID-19 participants; the 76 healthy controls in the original multicentre dataset were excluded by study design. Among the 572 participants, 145 (25.3%) had impaired DLCO, while 427 (74.7%) had normal DLCO. Compared with patients with normal DLCO, those with impaired DLCO were older, had a higher proportion of males, and had lower values of FVC, FEV1, and TLC (p < 0.05 for all comparisons). In contrast, weight, height, BMI, and FEV1/FVC ratio did not differ significantly between the two groups (p > 0.05).
Univariable logistic regression analysis identified several factors significantly associated with impaired DLCO (Table 2). Increasing age was associated with higher odds of impaired DLCO (OR 1.027 per 1-year increase; 95% CI 1.012-1.042; p < 0.001). Female sex was associated with lower odds of impaired DLCO (OR 0.489, 95% CI 0.330-0.725, p < 0.001). Higher FVC (OR 0.513, 95% CI 0.410 - 0.642, p < 0.001), FEV1 (OR 0.429, 95% CI 0.327 - 0.563, p < 0.001), and TLC (OR 0.684, 95% CI 0.573 - 0.817, p < 0.001) were each significantly associated with reduced odds of impaired DLCO. In contrast, BMI was not significantly associated with impaired DLCO (OR 1.018, 95% CI 0.983-1.054, p = 0.323). The FEV1/FVC ratio showed a borderline association but did not reach statistical significance (OR 0.117, 95% CI 0.010 - 1.323, p = 0.083).
A multivariable logistic regression model was used to identify independent factors associated with impaired DLCO (Table 3). The model included age, sex, and TLC, which were selected from candidate variables (age, sex, BMI, FVC, FEV1, and TLC) based on a combination of statistical criteria (p < 0.10 in univariable analysis) and clinical relevance informed by prior literature. This represents a reduced multivariable model due to exclusion of highly collinear pulmonary function variables. Variance inflation factor (VIF) values were assessed to evaluate potential multicollinearity among physiologically related variables. Age (VIF = 1.69) and sex (VIF = 1.11) demonstrated no evidence of multicollinearity, while TLC showed a low-to-moderate level (VIF = 3.04). In contrast, severe multicollinearity was observed for FEV1 (VIF = 121.15) and FVC (VIF = 110.69), reflecting their strong physiological interdependence; these variables were therefore excluded from the final model. After adjustment for covariates included in the model, older age remained independently associated with impaired DLCO, with each additional year increasing the odds (adjusted OR 1.025; 95% CI 1.009-1.040; p = 0.002). Female sex was statistically associated with lower odds of impaired DLCO compared with male sex (adjusted OR 0.379, 95% CI 0.247 - 0.583, p < 0.001). Higher TLC was also independently associated with lower odds of impaired DLCO (adjusted OR, 0.603; 95% CI, 0.493-0.738; p < 0.001).
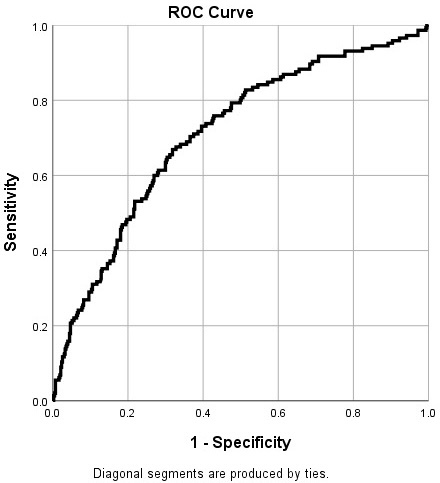
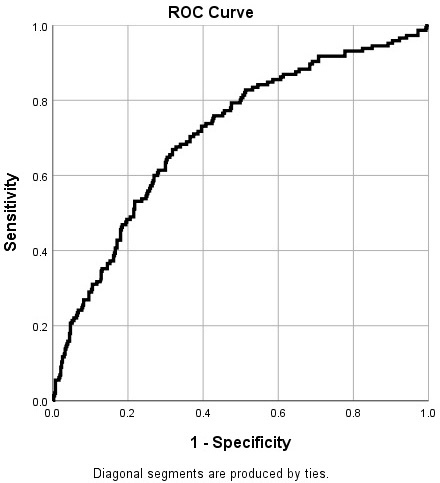
Model calibration was assessed using the Hosmer-Lemeshow test and showed no evidence of poor fit (χ² = 13.215, df = 8, p = 0.105). However, because no calibration plot was generated, calibration could only be partially evaluated and may not fully reflect agreement across the range of predicted probabilities. Discrimination was assessed using receiver operating characteristic (ROC) curve analysis (Figure 1). The area under the curve (AUC) was 0.710, indicating acceptable apparent discrimination in the development dataset.
Discussion
The main findings of this study indicate that age, sex, and TLC were statistically associated with impaired DLCO. Specifically, increasing age was associated with a higher likelihood of impaired DLCO, whereas higher TLC was associated with lower odds of impaired gas exchange. These findings should be interpreted as associations within secondary observational analysis rather than as causal or validated predictive effects.
Impaired DLCO has been widely reported as one of the most common pulmonary function abnormalities after COVID-19 infection.6,26,27 Prior studies have reported reduced DLCO in patients following COVID-19 infection, which may be associated with respiratory symptoms such as dyspnea and reduced exercise tolerance.28,29 Consistent with these reports, our findings indicate that a substantial proportion of patients recovering from COVID-19 in this cohort exhibited diffusion impairment. However, interpretation according to disease severity is limited due to the lack of stratified data.
Age was independently associated with impaired DLCO in the present analysis. This is consistent with prior studies showing that older individuals are more likely to have pulmonary function abnormalities after COVID-19.30,31 Age-related structural and physiological changes described in prior literature, including reduced alveolar surface area, decreased pulmonary capillary blood volume, and increased lung tissue stiffness, may be associated with reduced gas exchange capacity and could partially explain the observed association between age and impaired DLCO.30,31 However, these mechanisms were not directly assessed in the present study.32
The association between sex and impaired DLCO warrants cautious interpretation. In the multivariable analysis, female sex was statistically associated with lower odds of impaired DLCO after adjustment for potential confounders. It should be noted that impaired DLCO in this study was defined using GLI-based DLCO Z-scores, which are already adjusted for sex. Therefore, this association should not be interpreted as evidence of a direct biological protective effect of female sex. Rather, it may reflect sample composition, residual confounding, referral patterns, survivorship bias, or other unmeasured factors not fully captured in the dataset.33–35 Accordingly, the observed sex effect may reflect methodological and sampling factors rather than a true physiological difference in post-COVID gas transfer impairment. Further studies are warranted to better understand this association in different populations and analytic frameworks.
Another important finding of this study was the association between TLC and impaired DLCO. Lower TLC was independently associated with a higher likelihood of diffusion impairment, although this relationship should be interpreted as an association rather than a causal effect. TLC and DLCO may reflect related aspects of underlying pulmonary physiology, and their co-occurrence may indicate concurrent abnormalities rather than independent effects.27,36 Prior studies have described possible structural and vascular alterations following COVID-19 infection, including alveolar epithelial injury, interstitial inflammation, and pulmonary vascular abnormalities, which may be associated with reduced lung volumes and impaired diffusion capacity. However, these mechanisms were not directly evaluated in the present study and should therefore be considered speculative.36,37
The model demonstrated modest apparent discriminative performance, with an AUC of 0.71. However, this value was derived from the same dataset used for model development and therefore reflects apparent rather than validated performance. Because no internal validation (such as bootstrapping or cross-validation) or external validation was performed, the model’s true discriminative ability in other samples may be lower. Similarly, although the Hosmer-Lemeshow test did not suggest poor fit, calibration was only partially assessed, as this test alone does not provide a complete evaluation of calibration, and no calibration plot was available to assess agreement between predicted and observed probabilities across risk strata. Therefore, model performance should be interpreted cautiously. The present study has several strengths. The analysis drew on multicentre datasets and included a relatively large sample of post-COVID-19 patients who underwent standardized pulmonary function testing, which may improve the diversity of the study population across different clinical settings. In addition, the use of objective pulmonary function measures enabled a comprehensive assessment of lung function abnormalities in patients following COVID-19 infection. However, several limitations should be considered. This was a secondary, cross-sectional analysis, and available variables were limited to those collected in the original datasets, precluding assessment of longitudinal changes and detailed characterization of underlying mechanisms. In particular, the absence of radiological data, inflammatory biomarkers, and clinical symptom profiles limited the ability to classify the causes and clinical significance of impaired DLCO. In addition, incomplete information on the timing of pulmonary function testing relative to acute infection further constrains interpretation. Measurement variability may also have been introduced, as detailed information on hemoglobin correction and inter-site quality control for DLCO was not consistently available. In addition, because hemoglobin correction data were not consistently available, some participants may have been misclassified as having impaired DLCO when reduced diffusion capacity may have been partially attributable to hematological factors such as anemia. Accordingly, the reported prevalence of DLCO impairment may have been overestimated.
From an analytical perspective, the events-per-variable ratio during univariable screening approached the range in which unstable estimates and variable selection bias may occur. In addition, the use of univariable screening and the inclusion of physiologically related variables (e.g., FVC, FEV1, and TLC) may have introduced variable selection bias and multicollinearity; therefore, the model should be interpreted as exploratory and associational rather than as a validated clinical prediction model. Furthermore, the mechanism of missing data was not formally assessed, and participants with missing DLCO measurements or incomplete key covariate data were excluded, which may have introduced selection bias, particularly if missingness was related to disease severity or other clinical characteristics and may have influenced both prevalence estimates and observed associations. The exclusion of control subjects may also limit generalizability to the broader post-COVID population. Future studies incorporating longitudinal follow-up, imaging, biomarkers, and validated modelling approaches are warranted.
Conclusion
Impaired pulmonary diffusing capacity was observed in a substantial proportion of patients recovering from COVID-19. Age, sex, and total lung capacity were statistically associated with DLCO impairment in this secondary analysis. These findings should be interpreted as exploratory associations rather than causal or validated predictive effects. They should also be interpreted in the context of the limitations inherent to secondary complete-case analyses. Further prospective, severity-stratified, longitudinal, and externally validated studies are needed to clarify the clinical relevance and underlying mechanisms of DLCO impairment following COVID-19.
Contributions
Conceptualization, P. Amput; Methodology, P. Amput, W. Tapanya, N. Sangkarit, S. Ladawan and S. Wongphon; Formal Analysis, P. Amput; Data Curation, P. Amput; Writing, P. Amput; Original Draft Preparation, P. Amput; Writing-Review and Editing, P. Amput. All authors have read and agreed to the published version of the manuscript.
Conflicts of interest
All authors have completed the ICMJE uniform disclosure form and declare no conflict of interest.
Ethical approval
As a secondary analysis of de-identified multicentre datasets, no additional patient contact occurred. Ethical approval and informed consent were obtained in the original studies from which the datasets were derived.
Funding information
This research was supported by University of Phayao and Thailand Science Research and Innovation Fund (Fundamental Fund 2026, Grant No. 2264).
AI Statement
After completing the first draft of the manuscript, the authors used ChatGPT (OpenAI) to assist with improving the readability and language of minor sections of the manuscript. The AI tool was used solely for language editing purposes. Following the use of this tool, the authors carefully reviewed and revised the text as necessary and take full responsibility for the accuracy and integrity of the content of the publication.