
Introduction
Handheld positive pressure devices are commonly used in the clinical setting to increase lung volume, improve gas exchange and clear airways of secretions among people with acute and chronic lung conditions.1 These devices generate positive expiratory pressure that alters breathing patterns, decreases respiratory frequency and prolongs expiration, which can increase lung volumes, leading to an increase in functional residual capacity and improved gas exchange.1–4 Therapeutic expiratory pressures between 5-20 cmH2O have been demonstrated to improve forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), respiratory muscle strength, and reduce postoperative complications, including pneumonia and prolonged hospital stay.5,6
Although the observed positive physiological effects of handheld pressure devices are focused mostly on devices that create positive expiratory pressure, few are capable of creating both positive inspiratory and expiratory pressure. The EzPAP system (ICU Medical, San Clemente, CA, USA) is one such handheld device commonly used in Australian hospitals. It is proposed to increase tidal volume (VT) and functional residual capacity by augmenting inspiratory flow and generating positive expiratory pressure.7–10 During inspiration, the device amplifies airflow, potentially increasing inspired volume,10,11 while during expiration, the positive expiratory pressure generated by exhaling against the incoming flow may splint and stabilize the small airways, promote alveoli expansion, and ultimately enhance gas exchange.8
Despite its clinical use, evidence describing the physiological effect of the EzPAP remains limited.10,12–14 Prior studies have primarily relied on chest radiography, pulse oximetry and auscultation to evaluate its impact8,10,14 and the effect of EzPAP on tidal volume (VT) has not yet been quantified. Although reductions in respiratory rate have been reported,9,11,12 it is unclear whether minute ventilation (VE) is maintained during use. Additionally, the flow rates required to achieve therapeutic pressure levels have not been established.
Considering the primary proposed clinical populations for EzPAP are those with low lung volumes, such as postoperative or respiratory-impaired patients, and that its proposed mechanism relates to improving lung volumes to treat atelectasis, understanding how different flow settings influence lung volumes and airway pressures is essential. This study, therefore, aimed to determine whether the EzPAP achieves therapeutic pressure levels (>5 cmH2O) across different flow settings (flowEzPAP) and to evaluate the subsequent changes in VT and VE. The study was conducted in the healthy population to also observe for safety and tolerability, including user discomfort. The specific research questions were as follows:
-
What was the effect of flowEzPAP on VT in healthy adults?
-
What was the effect of flowEzPAP on VE in healthy adults?
-
What peak inspiratory pressures (PIP), peak expiratory pressures (PEP), as well as positive end-expiratory pressure (PEEP) were generated during EzPAP use in healthy adults?
-
How did the pressures influence VT and VE during EzPAP use in healthy adults?
-
What physiological changes, including heart rate (HR), blood pressure (BP), oxygen saturation (SpO2), respiratory rate (RR), rate of perceived exertion (RPE) and pain scores, occurred during EzPAP use in healthy adults?
Methods
Study design and setting
A prospective, observational, repeated-measures study was conducted in the research laboratory at Western Sydney University. Participants were blinded to the administered flowEzPAP. Ethics approval was obtained from Western Sydney University Human Research Ethics Committee (H14348), and all participants provided written informed consent.
Participants
Adults aged 18-70 years were recruited from the university community between April 2022 and May 2024. Participants were pre-screened with spirometry (EasyOne Diagnostic Spirometer, NDD Medical Technologies, Zurich, Switzerland) and included if their spirometric values indicated healthy adults, considered as ≥ 80% of the predicted spirometry values for their age, gender, ethnicity and height; could safely participate in physical activity as determined by the Physical Activity Readiness Questionnaire for Everyone (2021 PAR-Q+); have not had any recent significant surgery or trauma, illness or acute respiratory infection in the past 6 weeks; and were a non-smoker. Participants were excluded from the study if they had a medical diagnosis of any respiratory condition impairing lung function; a self-reported thoracic pain score of > 3 on the visual analogue scale (VAS); body mass index > 35; health conditions impairing accurate device usage, e.g. facial palsy or cognitive impairment; or inability to consent or understand English.
Equipment setup
A mouthpiece and bacterial filter were connected to a pneumotachometer heated to 37°C (Hans Rudolph Heated Series 3813 and Heater Control Series 3850AF, Hans Rudolph, Shawnee, Kansas). A short length of tubing connected the EzPAP to the pneumotachometer and pressure transducer (Hans Rudolph Pneumotach Amplifier 1, Series 1110, Hans Rudolph, Shawnee, Kansas). A flow of gas (medical air) was delivered via a calibrated flow meter (Ezi-Flow Flowmeter and Series-O Regulator, COMWELD Healthcare, Preston, Victoria) from a compressed gas tank through the gas flow port of the EzPAP.
Calibration of the pneumotachometer and pressure transducer was performed before each session using standard reference procedures.15,16 Flow and pressure signals were digitized, and a line of best fit was calculated using the data acquisition software, LabChart 8 (ADInstruments Pty Ltd, Bella Vista, NSW). For baseline measurements, the EzPAP and medical air gas flow were removed from the setup.
Protocol
Participants had a 5-minute seated rest in a relaxed upright position prior to baseline data measurements. During this rest period, the participants were orientated to the EzPAP and permitted to have a brief practice with feedback from the researcher when breathing technique required correction.
The participants were then instructed to remain seated, attach a nose clip, and perform tidal breathing through the mouthpiece for 60 seconds. Data collected at this stage was considered baseline data.
The EzPAP system and gas tubing were then connected and the participants were instructed to perform tidal breathing for 60 seconds for each of the following flowEzPAP. FlowEzPAP of 0, 5, 7, 9, 11, 13 and 15 L/min of medical air were delivered in a randomized order using a web-based computer-generated sequence (www.randomizer.org). These flow settings were selected to include a zero-flow condition as an internal comparator and to reflect manufacturer-recommended operating flows (5-15 L/min), allowing responses to be examined across the device’s practical operating range. A minimum rest period of one minute was provided between each flowEzPAP, with participants remaining seated until breathing pattern and physiological parameters had stabilized before commencing the next flowEzPAP. The flow meter was concealed to maintain participant blinding, although airflow noise at higher flowEzPAP could not be completely eliminated. Participants were instructed to breathe according to the manufacturer’s instructions, i.e., ‘breathe easily against the pressure from the device’. At flowEzPAP where the participant could not maintain tidal breathing, they were instructed to adapt their breathing technique to maintain what they perceived as a comfortable pattern of breathing with the instructions ‘breathe in a way you feel is most comfortable to synchronize with the device’. Each flowEzPAP was administered twice in a randomized sequence, and the full protocol was repeated in a second session, in line with recommendations that PEP therapy be repeated multiple times in clinical practice.5,17
Outcome measures
Participant demographics of age, sex, height, weight and ethnicity were collected prior to commencing the protocol.
Primary outcomes were VT and VE. Secondary outcomes included PIP, PEP and PEEP. A negative PIP indicated inspiratory effort performed by the participant, and a positive PIP indicated augmentation of the EzPAP. PEP was indicated by the maximum pressure at any time point during the expiratory phase, whereas PEEP was the pressure at the end of expiration. All volume and pressure measurements were recorded and extracted using the data acquisition software, LabChart8 (ADInstruments Pty Ltd, Bella Vista, NSW).
Physiological data, including HR and SpO2, were recorded via a finger pulse sensor and oximeter, respectively (Finger Pulse Transducer TN1012/ST and Oximeter Pod ML320/F, ADInstruments Pty Ltd, Bella Vista, NSW). The BP was measured via a manual blood pressure sphygmomanometer, and RR was recorded via LabChart 8. Dyspnoea, measured as RPE on a scale of 0-10 using the Modified Borg Scale18 and pain/discomfort scores measured on a scale of 0-10 using the visual analogue scale (VAS)19,20 were also recorded. All outcome data were collected at baseline. Volume and pressure data were recorded continuously and extracted from the 15th - 45th second window of each breathing period to allow for settling in and potential fatigue. Physiological data, as well as dyspnoea and pain/discomfort scores, were recorded immediately after each 60-second breathing period. Any symptoms or adverse events experienced by the participants were manually recorded with a time stamp for reference against the physiological data collected.
Statistical analysis
Based on an initial regression analysis of 10 participants, a total sample of 26 participants was required to detect a change in VT to allow confidence in the analysis of associations between flowEzPAP and VT at a power of 80%, with a medium effect size of 0.5 and 95% confidence interval. Data analyses were conducted using Statistical Package for Social Sciences (SPSS 29, IBM Corp., Chicago, IL). Participant characteristics were reported using descriptive statistics (mean ± standard deviation). Given the repeated measures study design, with multiple observations collected from each participant across different flowEzPAP conditions, generalized linear mixed models (GLMMs) were used to evaluate all outcomes in this study. FlowEzPAP was specified as a fixed effect, and participant was included as a random effect to account for within-participant correlation. Outcomes were modelled assuming a Gaussian distribution with an identity link function. Model assumptions were assessed by inspection of residual distributions. Robust (Huber-White) standard errors were applied to reduce sensitivity to deviations from normality and heteroscedasticity. Statistical significance was set at p < .05.
Results
Participant characteristics
All 26 screened participants were eligible and completed the study with no dropouts or withdrawals. All data were included in the analysis. Baseline demographics and physiological measures demonstrated normal spirometry and stable resting physiological parameters prior to testing (Table 1).
Effect of FlowEzPAP on VT
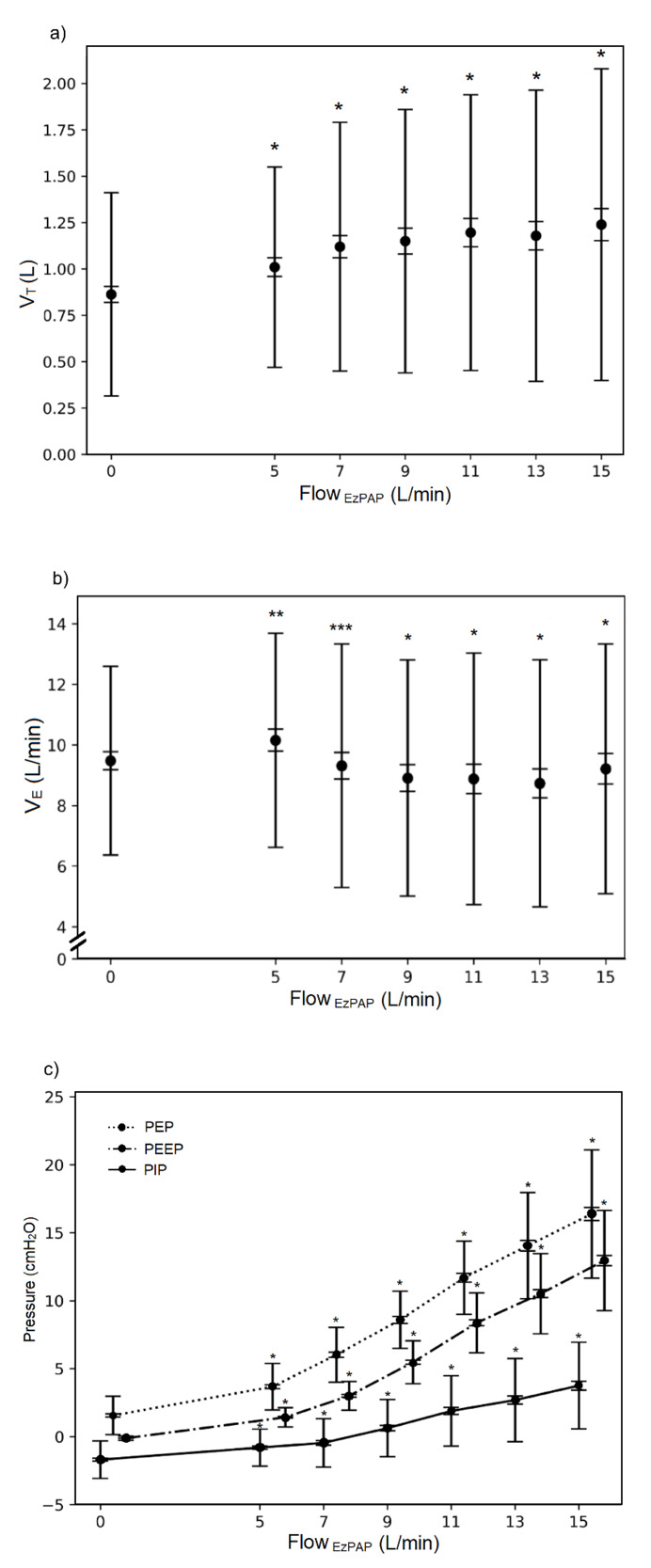
Increasing flowEzPAP produced a significant rise in VT (Figure 1a). The greatest mean difference was observed at flowEzPAP of 15 L/min, with a mean increase of 0.35 L compared to zero flowEzPAP (p < .001, 95% CI: 0.29 to 0.41). Variability of the data increased at the higher flowEzPAP. Each 1 L/min increase in flowEzPAP predicted a 0.02 L increase in VT, described by VT = 0.93 + 0.02 x flowEzPAP (p < .001, 95% CI: 0.02 to 0.03).
Effect of FlowEzPAP on VE
VE decreased significantly as flowEzPAP increased (Figure 1b). The greatest mean reduction was observed at flowEzPAP of 13 L/min, with a mean decrease of 0.84 L/min compared to zero flowEzPAP (p < .001, 95% CI: 0.48 to 1.20). Variability increased at flowEzPAP ≥ 7 L/min. Each 1 L/min increase in flowEzPAP predicted a 0.07 L/min reduction in VE, described by VE = 10.50 – 0.07 x flowEzPAP (p < .001, 95% CI: -0.10 to -0.05).
Effect of FlowEzPAP on PIP, PEP and PEEP
PIP, PEP and PEEP increased significantly as flowEzPAP increased (Figure 1c). The variability of the data also increased as flowEzPAP increased, with expiratory pressures of PEP and PEEP showing the greatest magnitude of change.
The highest mean PIP was observed at flowEzPAP of 15 L/min (3.75 cmH2O, SD = 3.20) and was associated with the greatest mean increase of 5.40 cmH2O compared to zero flowEzPAP (p < .001, 95% CI: 5.18 to 5.61). The PIP was positive at flowEzPAP >7 L/min. Each 1 L/min increase in flowEzPAP, predicted a 0.37 cmH2O increase in PIP, described by PIP = -2.23 + 0.37 x flowEzPAP (p < .001, 95% CI: 0.35 to 0.38).
The highest mean PEP was observed at flowEzPAP of 15 L/min (16.37 cmH2O, SD = 4.71) and associated with the greatest mean increase of 15.06 cmH2O compared to zero flowEzPAP (p < .001, 95% CI:14.74 to 15.38). Each 1 L/min increase in flowEzPAP predicted a 1.04 cmH2O increase in PEP, described by PEP = -0.24 + 1.04 x flowEzPAP (p < .001, 95% CI: 1.02 to 1.05).
The highest mean PEEP was observed at flowEzPAP of 15 L/min (12.95 cmH2O, SD = 3.69) and associated with the greatest mean increase of 13.33 cmH2O compared to zero flowEzPAP (p < .001, 95%CI: 13.09 to 13.56). Each 1 L/min increase in flowEzPAP predicted a 0.91 cmH2O increase in PEP, described by PEEP = -1.90 + 0.91 x flowEzPAP (p < .001, 95% CI: 0.90 to 0.92).
Relationship between changes in VT and VE and pressure variables
After allowing for the correction of variances of the flowEzPAP and pressure variables themselves, both PIP and PEP were determined to be significant predictors to VT (p < .001), whereas PEEP was not (Table 2). All pressures, PIP, PEP and PEEP were significant predictors to VE (p < .001) (Table 3).
Effect on physiological outcomes
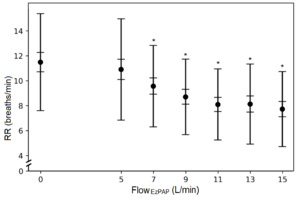
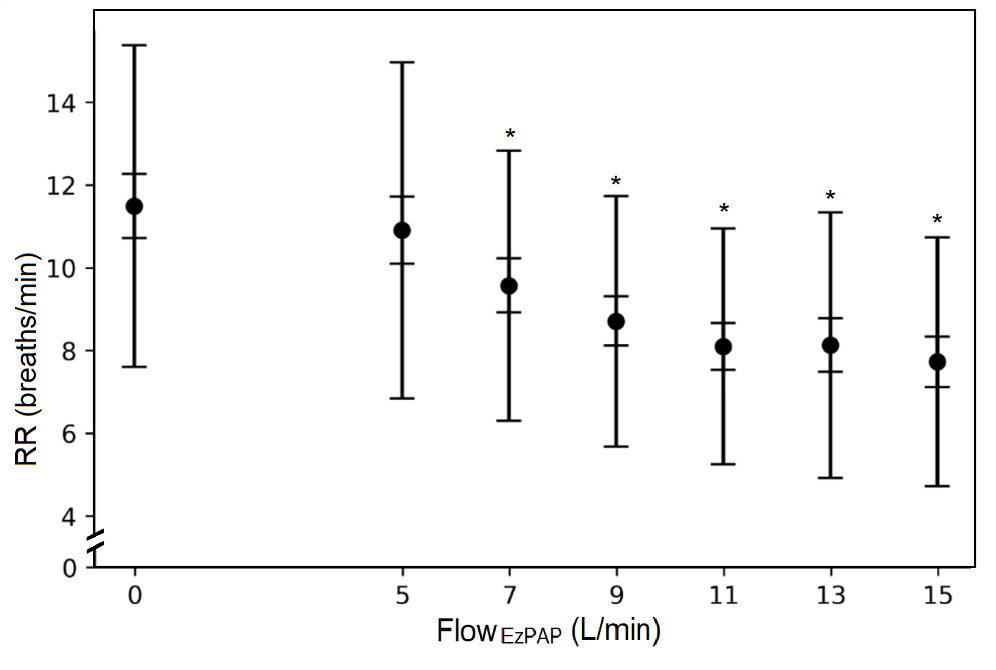
Overall, HR, BP (both systolic and diastolic) and SpO2 remained statistically and clinically unchanged across flowEzPAP (p = .058, p = .164, p = .794 and p = .764, respectively). The RR decreased significantly with increasing flowEzPAP (Figure 2), with the greatest variability at flowEzPAP ≤ 5 L/min. The greatest mean reduction in RR was 3.88 breaths/min (p < .001, 95% CI: 3.13 to 4.62).
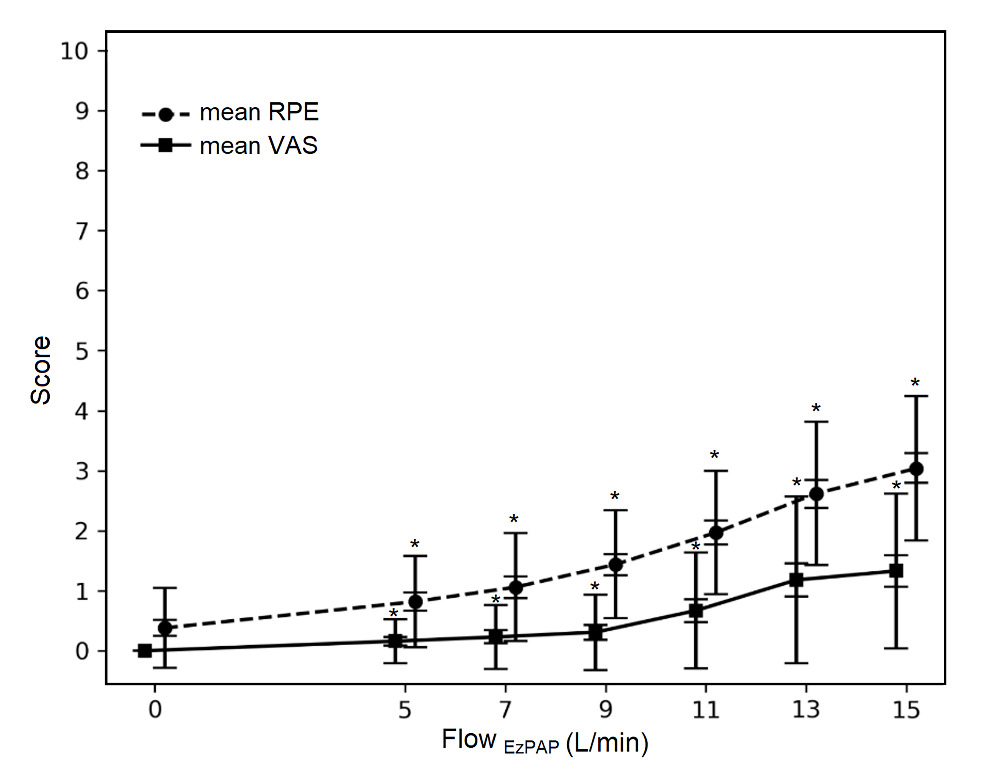
Effect on user tolerability
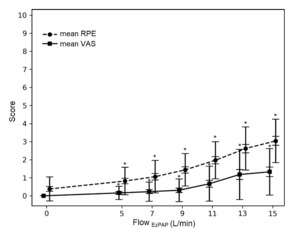
Both RPE and VAS increased with increasing flowEzPAP (Figure 3). Variability of the data increased at the higher flowEzPAP. For RPE, the greatest mean difference was 2.65 out of 10, described as less than ‘moderate’ level of exertion (p < .001, 95% CI: 2.43 to 2.89). For VAS, the greatest mean difference was 1.33 out of 10, described as mild pain or discomfort (p < .001, 95% CI: 1.12 to 1.54). The highest RPE and VAS reported by any participant was 6 out of 10. Difficulty adapting breathing and cheek discomfort were more common at flowEzPAP of ≥ 13 L/min. At flowEzPAP of 15 L/min, eight participants reported difficulty with adapting their breathing. Six participants reported discomfort in the cheeks. No participants reported any pain or discomfort in their chest whilst using the EzPAP. All reported discomforts and difficulty with breathing were completely resolved during the rest periods.
Adverse event
One participant experienced transient light-headedness associated with a 10 mmHg drop in systolic BP at flowEzPAP 15 L/min, resulting in SBP < 90 mmHg. Symptoms resolved with a return of SBP to baseline with immediate cessation of breathing at this flowEzPAP. There were no other adverse effects reported in the study.
Discussion
This study is the first to rigorously examine the physiological effects of the EzPAP system on healthy adults, demonstrating that the device significantly increased resting VT and generated clinically relevant positive airway pressures across a range of flowEzPAP. At the highest flowEzPAP, the VT inhaled almost doubled the expected resting VT for a healthy adult,21 supporting the device’s proposed mechanism of increasing lung volumes, a key therapeutic goal in populations at risk of atelectasis. In this healthy cohort, the device was generally well tolerated with only one transient adverse event. These findings provide foundational evidence for establishing safety and therapeutic benefits in the healthy population. However, further studies are required to establish therapeutic benefits in clinical populations.
The likely mechanism for increasing VT relates to the increasing pressure changes generated when flowEzPAP increased. The pressure differentiation between inspiration and expiration is theorized to create a splinting effect that stabilizes the small airways from collapsing, with potential recruitment of alveoli, shearing of secretions and decreasing the work of breathing.1,22,23 The positive expiratory pressure component of EzPAP plays a crucial role by potentially increasing functional residual capacity, enhancing alveolar stability and expanding the surface area available for gas exchange. By maintaining end-expiratory lung volumes, the EzPAP potentially reduces ventilation-perfusion mismatch and supports more efficient oxygenation.1,14 These physiological effects align with previous clinical studies demonstrating improved respiratory mechanics and oxygenation with EzPAP use.8,9,12–14,24 Furthermore, the increasing positive inspiratory pressure at higher flowEzPAP may have overcome airway resistance, enabling greater inspired volume which in return facilitated the reduction in work of breathing.25 As such, there is potential for EzPAP to positively impact outcomes in clinical populations at risk of atelectasis, such as those following thoracic surgery or trauma.26
A key finding of this study is the identification of threshold flow rates required to achieve therapeutic expiratory pressures. It is important to note that clinically therapeutic expiratory pressures (> 5 cmH2O)5,27 did not occur until flowEzPAP exceeded 7 L/min for PEP and 9 L/min for PEEP in this healthy cohort. These thresholds are clinically relevant, as pressures exceeding this threshold have been associated with airway stabilization during expiration, although lower pressures may still be clinically meaningful depending on patient characteristics and therapeutic goals. Furthermore, a PEEP of 5 cmH2O has been demonstrated that the splinting effect increases alveolar surface and improves alveolar recruitment creating more areas for gas exchange and possibly improving ventilation.28 Previous clinical studies demonstrated therapeutic pressures with EzPAP, but did not specify the flowEzPAP thresholds required.8,12,14,29 It is important to note that the findings from our study may not directly translate to the clinical population due to differences in lung compliance related to pathophysiological processes. However, the present findings offer an important reference point for understanding the threshold flowEzPAP for the EzPAP to generate therapeutic pressure levels in different clinical sub-groups for the prevention or reversal of atelectasis.
In this healthy adult sample, the EzPAP was generally well tolerated, The pressures achieved were well below the levels required to induce barotrauma (> 35 cmH2O).30,31 These findings indicate that the airway pressures generated across the tested flowEzPAP range remain within safe physiological margins for healthy adults.
Although VE decreased with increasing flowEzPAP, the observed values remain within physiologically acceptable ranges for healthy adults and were not associated with changes in SpO2, HR, or BP. In this context, the reduction in VE likely reflects a change in breathing pattern characterized by increased tidal volume and a reduction in respiratory rate, rather than clinically meaningful hypoventilation. However, these findings reflect only healthy individuals, and a similar response may be less well tolerated in clinical populations with reduced respiratory reserve, impaired respiratory drive, or altered lung mechanics. As such, while the magnitude of VE reduction observed in this healthy cohort appears acceptable, close monitoring of physiological responses would be required for the clinical population until safety can be established.
While there were statistically significant increases in RPE and VAS with increasing flowEzPAP, the mean scores reported in the healthy population do not exceed a rating of 3, indicating moderate exertion and mild discomfort or pain.18–20 Higher ratings for RPE and VAS up to 6 occurred at flowEzPAP ≥ 13 L/min corresponding to ‘hard’ on the Borg scale18 and moderate discomfort or pain.20 This only occurred prior to any correction of breathing technique when tidal breathing could not be maintained. This highlights that tolerability at higher flowEzPAP is influenced by an individual’s ability to adapt their breathing pattern to the device. While these effects resolved during rest periods in healthy adults, clinicians should be cautious when prescribing the EzPAP in the clinical population, where synchronizing breathing with the device may be more challenging. Clinicians should consider providing very specific instructions for use and actively observing breathing patterns, with feedback for correction, to support patients in learning to use the device accurately and minimize the likelihood of discomfort.
There was only one transient adverse event that occurred, where a participant felt lightheaded as a result of a drop in blood pressure and needed to cease using the EzPAP. The participant’s blood pressure returned to baseline values within a 5-minute rest period. Of note, the participant had a resting systolic blood pressure of 95 mmHg prior to commencing testing, suggesting that individuals with borderline hypotension may be more susceptible to such responses. This finding underscores the importance of detailed monitoring of physiological parameters during EzPAP use and reinforces that safety observed in healthy adults cannot be assumed to translate to clinical populations with cardiovascular or respiratory compromise.
There are several limitations to this study that warrant consideration in interpretation of the findings. Firstly, participants were blinded to the flowEzPAP administered, but increasing airflow noise at higher flowEzPAP could not be eliminated. The increased noise provided a differentiation of higher and lower flowEzPAP possibly leading to pre-determined changes of patterns of breathing anticipated by the participant.
Secondly, the 0 L/min condition required participants to breathe through the EzPAP device and mouthpiece assembly, which introduces resistance not present during unobstructed spontaneous breathing. This resistance may have influenced respiratory pattern and the measured outcomes at this setting. As such, this condition should be interpreted as an internal comparator within the experimental setup rather than a true representation of normal tidal breathing.
Additionally, it was possible that participants had prior knowledge about physiological impacts of breathing as recruitment of the general population included health professionals and academics at the University. Having prior knowledge of the impact could have changed their behaviour or breathing patterns throughout the study and potentially affected the outcomes. Nevertheless, irrespective of participants’ prior knowledge of respiratory mechanics, the more active breathing pattern required to accommodate higher flowEzPAP with EzPAP likely meant that the VT recorded did not reflect true tidal volumes but rather represented augmented inspired volumes. The present findings likely reflect real-world use and do not diminish the relevance of the findings.
Finally, the large variability of volumes and pressures found in this study suggest that translating any significant effects of the EzPAP to improve VT in the clinical population should be approached cautiously. Whilst participants were initially given standardized instructions in breathing technique to minimize the variability of the data, the large variety of different breathing patterns found amongst the healthy participants highlights the need for carefully considered instructions in clinical populations.
Conclusion
This study examined how different flowEzPAP settings influence tidal volume, minute ventilation, airway pressures and associated physiological responses in healthy adults, and evaluated how pressures changes contributed to changes in VT and VE. Increasing flowEzPAP produced clinically relevant increases in tidal volume and airway pressures, while the reduction in VE was small and unlikely to be clinically significant in this population. Therapeutic levels of expiratory pressure were achieved at flowEzPAP above 7 L/min. The large variability in volumes and pressures indicates that translating these findings to clinical populations should be approached with caution. As the study was conducted exclusively in healthy adults with normal lung mechanics, the safety and physiological responses observed here cannot be assumed to apply to clinical groups with reduced lung volumes, altered lung compliance, or hemodynamic instability. Nevertheless, these findings provide foundational evidence describing how EzPAP flow settings influence lung volumes and airway pressures and indicate safe for use in healthy adults. Further research is warranted to determine whether similar effects occur in clinical populations at risk of atelectasis, such as those following thoracic surgery or thoracic trauma.
Acknowledgements
The authors thank Dr. Paul Fahey for statistical consultation.
Author Disclosure Statement
All authors have completed the ICMJE uniform disclosure form and declare no conflict of interest.
Funding source
The consumables used in this study were funded by Western Sydney University’s Research Training Program. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval and informed consent statement
This study was approved by the Western Sydney University Human Research Ethics Committee (H14348, approved 8 July 2021). All participants provided written informed consent prior to participation.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
AI Statement
The authors confirm no generative AI or AI-assisted technology was used to generate content.