Introduction
Chronic respiratory diseases (CRD), such as chronic obstructive pulmonary disease (COPD), asthma and pulmonary fibrosis, impact millions of people around the world, with COPD being the most frequently encountered diagnosis.1 COPD predominantly affects individuals over the age of 55 and is characterized by progressive bronchial obstruction accompanied by an inflammatory process that reduces airflow.2 Individuals with chronic respiratory disease experience additional health issues, such as shortness of breath (dyspnea) and reduced quality of life.1 Dyspnea has been shown to affect communication, notably through decreased speech fluency.3 Furthermore, people with pulmonary disease, especially COPD, can also experience cognitive decline.4 COPD symptoms can reduce mobility and increase difficulties in planning complex or new activities, which can significantly affect daily life.5 Finally, as the illness progresses, symptoms often lead to social isolation by limiting opportunities for social participation.6,7
Pulmonary rehabilitation (PR) is known as the cornerstone treatment for patients with CRD, and has been proven effective in reducing the impact of pulmonary symptoms.8,9 However, access to PR is limited due to a shortage of resources, making it difficult to provide it for everyone who may need it. As a result, PR is often underprescribed and underused.10 Moreover, several studies have shown that the benefits obtained during PR tend to diminish within six months to one year after its completion.11–13 These findings highlight the need for alternative and sustainable interventions to help this population remain active and socially engaged over the long term.
Innovative group singing (GS) programs have emerged as a promising option to address both the respiratory and psychological needs of patients with CRD.14 GS is accessible, easy to set up, and does not require a team of healthcare professionals or expensive equipment.15 Previous studies on in-person GS with older adults have reported various benefits, including reduced symptoms of anxiety and depression,7,16,17 improved quality of life,18–20 and better cognitive function.21 Singing is characterized by increased expiratory control and longer maximum phonation time, reflecting greater engagement of expiratory muscles.22,23 In individuals with chronic pulmonary disease, respiratory muscle dysfunction is reflected by reduced maximal respiratory pressures.24 Bonilha et al. observed a significant improvement in maximum expiratory pressure (PeMax) in a singing group following weekly singing sessions over 24 weeks, compared with a control group engaged in handicraft activities. PeMax is an indirect indicator of respiratory muscle strength, assessed by measuring pressure at the mouth using a handheld pressure meter or manometer.25 These findings support the physiological rationale by which singing practice enhances respiratory muscle function, as reflected by improvements in PeMax, in individuals with chronic respiratory disease.26 A large randomized controlled trial suggests that GS was non-inferior to PR in improving functional exercise capacity, as measured by the 6-minute walk test.18 GS has also been found to decrease social isolation.7
Although the results are promising, in-person group singing may limit participation due to travel distance, discomfort or anxiety about singing in front of others,27 and concerns about the risk of infection associated with close contact with other participants. The online modality thus emerges as a valuable alternative for making group singing more inclusive.28 Online GS during the COVID-19 pandemic has been shown to decrease symptoms of depression, improve balance confidence, and enhance participants’ perception of their breathing ability.28 Additionally, the same research team demonstrated that online GS was safe and well-tolerated by patients with CRD.29 To the best of our knowledge, no study has documented a hybrid delivery mode combining in-person and online modalities simultaneously. It is essential to offer an alternative, such as online participation, for people who are unable to attend in person for various reasons, including distance, transportation issues, or health concerns, while maintaining the in-person group. However, it remains unclear whether interactions between these two groups influence the program’s effectiveness or the participants’ experience.
Our study aims to explore participants’ experiences and the effects on respiratory control, quality of life, and social inclusion of a hybrid GS program that includes in-person and online groups simultaneously.
Methods
We conducted a pilot study using a mixed-method convergent design. This design combines quantitative and qualitative data to provide a more complete understanding of the group singing intervention.30 The study was approved by the research ethics committee (#2023-4921) of the Centre Intégré Universitaire de Santé et de Services Sociaux de l’Estrie – Centre Hospitalier Universitaire de Santé de Sherbrooke (CIUSSS de l’Estrie – CHUS). The intervention was conducted in spring 2023. We report our data in accordance with the Mixed Methods Article Reporting Standards.31
Participants and recruitment
The recruitment strategies involved convenience sampling from a list of potential participants identified through the CHUS pulmonology outpatient clinic and the use of posters displayed in the clinic’s waiting areas. The recruitment was also carried out by two community organizations: SERCOVIE, a non-profit organization that promotes recreational activities and provides in-home support for seniors, promoted the hybrid GS interventions on their website; and the Quebec Lung Association (QLA), a non-profit organization dedicated to respiratory health. QLA promoted and invited their members from a post-PR exercise group to participate in the hybrid GS intervention.
Inclusion criteria were 1) participants aged 50 years or older; 2) having a lung disease or a breathing limitation (e.g., difficulties performing daily activities, dyspnea at rest or with low-intensity exertion) preventing from joining in community choirs; 3) having at least moderate dyspnea (≥2/5 on the Medical Research Council scale); and 4) being medically stable for at least four weeks prior to the study. The study took a community-based approach, focusing on individuals with breathing limitations instead of requiring a medical diagnosis. This decision was made to reflect real-world access issues, since obtaining a formal diagnosis is not always possible.
Exclusion criteria were 1) having a heart condition or other comorbidities that would interfere with safe participation; 2) having significant cognitive impairment (MoCA < 2 standard deviations)32; 3) having severe hearing problems with non-compensated hearing impairments; and 4) not understanding, speaking, reading, or writing French. The target sample size was 20 participants. This number is based on the CIFR model as a pragmatic guideline33 and a study by Lewis et al.34 To account for anticipated early withdrawals, we aimed to recruit 24 participants.
Hybrid group singing intervention
Participants met once a week, either in person or online via the Zoom platform. The in-person participants were mostly from the SERCOVIE network, and the online participants were mostly from the QLA organization. Those recruited from the QLA also participated in a once-a-week exercise maintenance program. In-person participants could choose to participate online if they wished or if their health condition did not allow them to participate in person, but in-person participation was strongly encouraged. The online participants could also attend the in-person sessions if they wished.
Participants were welcomed 15 minutes before the start of the session to allow time for socializing and any necessary adjustments to the online connection. A trained facilitator with experience in GS for seniors with respiratory limitations (LD) led physical warm-ups focusing on posture exercises and controlled breathing modelled after PR exercises, while adding vocal exercises. In addition, at the beginning of each session, participants self-rated their dyspnea using the Borg Modified Dyspnea Scale (0 to 10), and their measure of Forced Expiratory Time (FET) by exhaling for as long as possible with the /s/ sound and Maximum Phonation Time (MPT) by holding the /a/ sound as long as possible to self-monitor their progress. The group then sang for about 30 minutes, alternating between standing and sitting positions, followed by a 15-minute social break. The session concluded with an additional 45 minutes of singing for a total of 2 hours.
Music-making activities included listening, singing, playing small percussion instruments such as maracas (only for the in-person group), and performing simple movements such as upper body motions, hand clapping, and stepping. The repertoire included popular, folk, and classical songs selected to match the participants’ abilities and preferences and to encourage diaphragmatic breathing. When possible, participants’ favourite songs were included, and some vocal techniques and score-reading skills were taught. Polyphonic, canon, and a cappella added variety and challenges to the singing sessions. Materials provided included lyrics and sheet music, access to web links, and recordings. A pianist accompanied the group during most of the sessions.
For the online group, during singing segments, microphones were muted to manage latency and unmuted only when a participant was assigned to perform a solo or to ask a question. Participants of the online group could interact verbally during the welcome time, scheduled breaks, and at the end of sessions.
Qualitative data collection
To assess participants’ experience with the hybrid GS intervention, semi-structured interviews were conducted with a qualitative descriptive design.35 The interviews took place at the end of the intervention. They lasted between 18 and 107 minutes, were audio-recorded, and transcribed verbatim. The interviews were conducted either in person, online, or by phone by a research assistant who was not involved in the intervention.
The interview guide (see Supplementary Material) was designed to explore participants’ experiences and perceived effects of the program and was pilot tested with a community member. It was based on a PR satisfaction questionnaire for a previous work,14 from which we modified the questions to be more open-ended and refined the prompts to better align with the study objective. The interview guide focused on the participants’ real-life experiences, referring to the perceived effects on their health, and the advantages and disadvantages of both in-person and online delivery interventions. Five topics were covered: personal experiences with the program, the research team, perceived effects, perceptions of others, and looking to the future (see Supplementary Material). Questions related to perceived effects included participants’ reflections on pulmonary health, functional capacity, cognition (e.g., memory and concentration), quality of life, and social inclusion.
Quantitative data collection
Quality of life
Quality of life was assessed using two tools. First, the Subjective Units of Discomfort Scale (SUDS) is a 10-level scale that measures anxiety symptoms, with higher scores indicating a greater degree of anxiety/discomfort experienced by the individual. Correlations up to 0.74 show a fair validity for this scale.36 Second, the COPD Assessment Test (CAT) measures patient-reported symptoms that affect health-related quality of life.37 It is a scale between 0 and 40, where a score of less than 10 would have a minimal impact on quality of life, between 10 and 20 a moderate impact, between 21 and 30 a high impact and more than 30 a very high impact.38
Respiratory Control
To assess the potential effects of the intervention on respiratory control, two metrics were used: Forced Expiratory Time (FET) and Maximal Phonation Time (MPT). FET measures the duration a participant can sustain a single expiration, reflecting the strength and endurance of the expiratory muscles.39 It is measured using a task of sustained production of the sound /s/ (voiceless phoneme) during a single expiration. A member of the research team used a chronometer to announce each second aloud while participants sustained the sound /s/. When they could no longer produce an audible sound, they recorded individually the duration achieved. MPT measures the duration a participant can sustain phonation on a single expiration, indicating the efficiency of the vocal and respiratory systems working together to achieve sustained phonation.39 It is measured using a task of sustained production of the sound /a/ (voiced phoneme) during a single expiration. Both metrics were used to monitor progress during intervention. The MPT was performed using the same procedure as the FET.
Single breath counting (SBC) was also used to assess respiratory control. Participants were asked to take a deep breath and count aloud for as long as possible, with the total duration recorded in seconds.40 When formal lung function testing is not feasible, SBC is considered a highly sensitive indicator for low forced vital capacity (FVC).40
Social inclusion
Social inclusion was evaluated using two tools. First, the Positive and Negative Affective States (PANAS) scale is a widely used measure of mood and emotion.41 This scale shows high internal consistency, with largely uncorrelated and stable scores over appropriate periods. The complete version with 20 items was used.42
Second, the Inclusion of Other in the Self Scale (IOS) consists of a single item that measures how close an individual feels with another person or group. The tool contains seven diagrams, pairs of circles, that range from just touching each other to almost completely overlapping. It prompts individuals to reflect on which image best describes their relationship with a specific group/person and choose the diagram that best demonstrates the relationship.43
Data collection
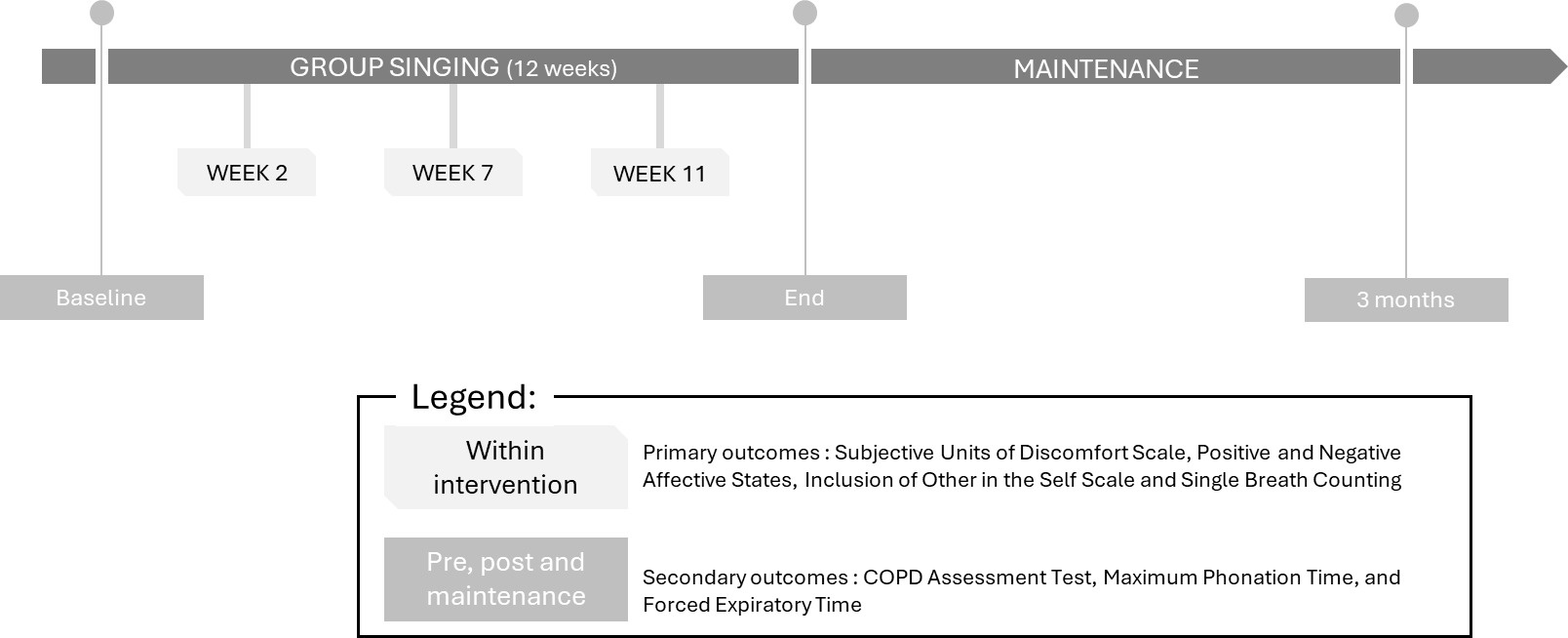
Data were collected at baseline, after the intervention (week 12), and three months later (pre-, post-, and maintenance), as well as during the intervention (weeks 2, 7, and 11) (see Figure 1). Demographic data, including gender, age, and educational level, were collected at baseline.
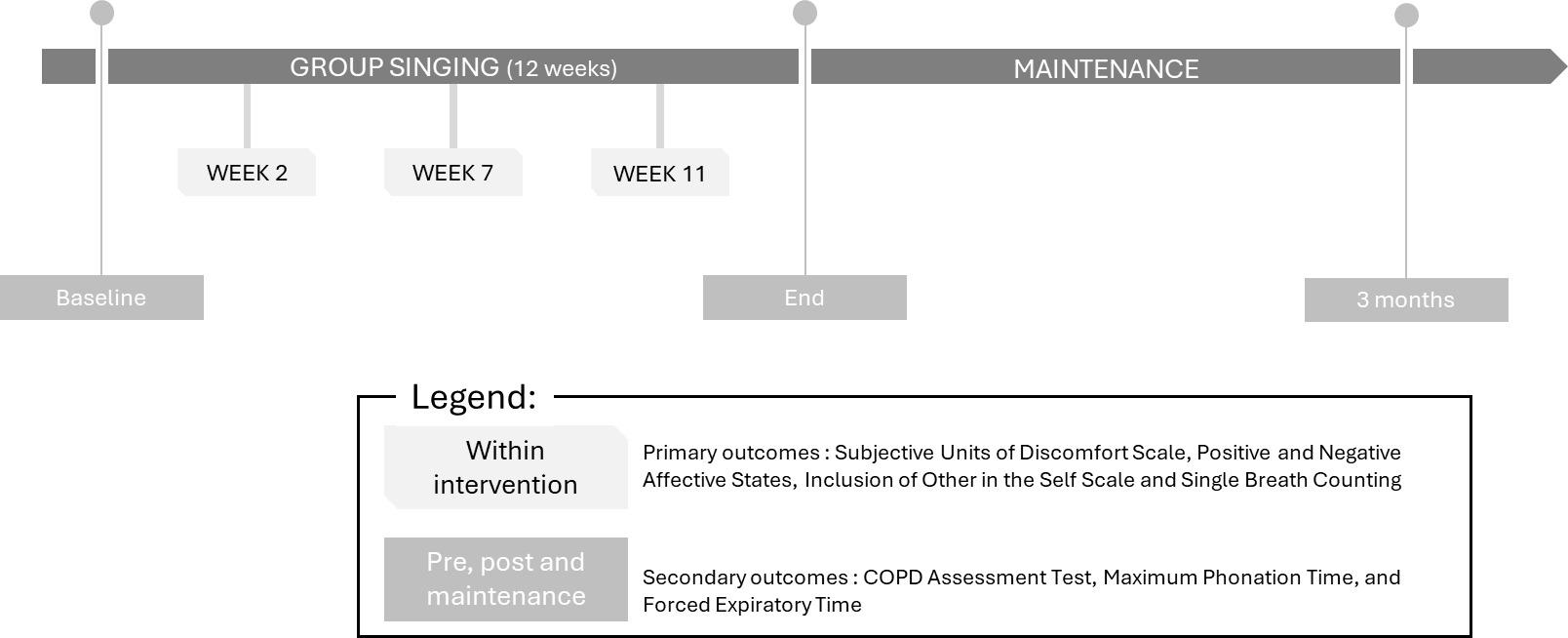
The outcomes within the intervention were used to monitor progression of respiratory control, quality of life, and social inclusion during the intervention, and they were measured by the SBC, SUDS, PANAS, and IOS. Data were collected at three time points: week 2, week 7, and week 11, in collaboration with the SingWell program from Toronto Metropolitan University.
The pre-, post- and maintenance outcomes were collected to assess quality of life and respiratory control over a longer period. These measures, added by our research team, included the CAT for quality of life, and temporal metrics of respiration (FET and the MPT) for respiratory control. This data was collected before the start of the intervention, after the intervention and three months later for maintenance.
Analysis
Qualitative data analysis
A content analysis was conducted. Transcripts of all interviews were compared to the audio files, and any discrepancies were corrected. All transcripts were anonymized by removing any names or locations that could identify participants. Two people (JL and LD) read the transcripts and coded them independently.44 A table was created containing the previously identified categories for each participant. The categories were selected based on the study’s objectives and participants’ responses, and themes were developed as the analysis progressed. When a new category was created, the authors revisited the previously analyzed transcripts to identify information that could be included in it. Co-validation of the analysis was performed when the table from JL and LD was compared. Any disagreements between JL and LD were resolved by discussion. If disagreements remained, a third author (NM) helped resolve them.
To further strengthen credibility, the other authors served as peer reviewers throughout the study, meticulously examining and consistently questioning the analytical process and interpretation of the results. All participants were included in qualitative interviews to enhance the study’s validity. Additionally, verbatim excerpts were translated into English during manuscript preparation, and each translation was reviewed and validated by at least two authors.
Quantitative data analysis
To describe the sample, categorical variables were summarized using counts and percentages, and continuous variables were presented as means and standard deviations. For the outcomes within the intervention, mean values and standard deviations were compared across the entire sample and separately for the online and in-person groups. Assessments occurred at weeks 2, 7, and 11. Given the small sample size (n < 30), the Wilcoxon signed-rank test for within-group comparisons was applied with a significance threshold set at 5%. Because both groups showed similar tendencies, we combined in-person and online participants into a single group to increase statistical power.
The outcomes measured before, after the intervention, and during the maintenance phase were evaluated using the same approach, examining data collected at baseline, post-intervention, and at a three-month follow-up, both overall and by delivery mode, to assess sustained effects.
Mixed methods analysis
Finally, both quantitative and qualitative results were compared and then combined to better understand the effect of the hybrid GS program.30
Results
Participants
We recruited 26 participants, with 14 primarily attending the in-person group and 12 in the online group. Six participants dropped out (two from the in-person group and four from the online group), leaving 20 participants who completed the intervention (12 in person and 8 online). Reasons for dropout included difficulties with technology (n = 3), health issues (n = 1), scheduling conflicts (n = 1), and withdrawal of consent to participate in the research project (n = 1). The sample were predominantly women (85%), with a mean age of 72.05 years (standard deviation = 6.26), and was educated, with 50% having completed university education (see Table 1). All participants were francophone except one, who was bilingual (anglophone), and all participants were retired except two participants who worked part-time. The majority of the participants had COPD (12/20), and the other participants had breathing limitations preventing them from joining a community choir. Participants in the in-person group attended an average of 97% of sessions (11.58/12). Seven participants occasionally joined online sessions (between one and four times). Participants in the online group attended 79.6% of the sessions on average (7.16/12), and only one participant attended in-person sessions on three occasions.
Participants’ experiences with the hybrid program
Various factors contributed to the participants’ experience of hybrid group singing. Firstly, following the COVID-19 pandemic, participants expressed concern about the risk of infection from any disease. They noted that being able to participate online allowed them to sing without fear of exposure: “If there was an epidemic, I would not go […] the advantage was that there was Zoom” (In-person-02). In addition, singing in front of others can be intimidating, and some participants reported feeling shy when singing in a group. They expressed that singing through Zoom allowed them to participate without worrying about others judging their voice: “It’s also less awkward since our microphones are muted.” (Online-3). Participants also mentioned the social connections they developed: “There are bonds that are formed […] like a little family” (In-person-04).
Certain aspects of the intervention itself also had an impact on participants’ experiences. They appreciated the duration and location of the sessions, as well as the choice of songs, although some participants expressed a preference for contemporary music: " I would have liked something more up to date" (Online-01). In addition, participants appreciated the musical guidance provided by experienced professionals and noted that this support enhanced their overall experience: “I thought it was great. I did not even expect to get that” (Online-01).
In-person and online participants expressed concerns about using the technology during the intervention. They noted that when technical problems arose, they could take a long time to resolve, which disrupted the flow of the sessions: “we had less practice, less singing, less progress” (In-person-04). In addition, online participants emphasized that they were unable to receive feedback on their singing performance when their microphones were muted, which had a negative impact on their experience. In fact, this lack of immediate feedback made it difficult for them to assess their accuracy and progress.
Both in-person and online participants had a positive experience with the group singing. Both groups reported a sense of connection with other participants, although online participants took longer to feel fully integrated into the group. Despite some concerns, online participants were grateful to have the opportunity to participate in this type of intervention: “If it had not been for Zoom, I would not have had the experience” (Online-07). Additionally, technological challenges impacted participants differently. In-person participants expressed dissatisfaction when technical issues disrupted the flow of the session, whereas online participants felt isolated because in-person participants could not hear them: “Give two minutes to [the online group] to be sure everything is alright. That way, we’ll feel more heard” (Online-09).
Effect of the group singing intervention
Outcome within the intervention
For all participants, there was a statistically significant difference between week 2 and week 11 in the SBC score (p = 0,017), with participants able to count 5 more numbers in 1 minute, suggesting a longer-lasting outbreath (see Table 2). This change primarily occurred between week 7 and 11 (p = 0,018). For the IOS, there was a statistically significant difference (p = 0,002) at week 11, indicating an improvement in social inclusion. This change primarily occurred between week 2 and 7 (p = 0,003). For the PANAS, there was a statistically significant difference (p = 0,010) at week 11 for the positive questions, showing improvement in affect such as enthusiasm, interest, and determination. The change primarily occurred between week 2 and 7 (p = 0,038). There was no difference for the negative questions on affects such as anxiety, fear and shame; however, their original scoring was already low. Finally, there were no changes in the SUDS, suggesting no change in the degree of discomfort and anxiety.
Outcome pre-, post- and maintenance
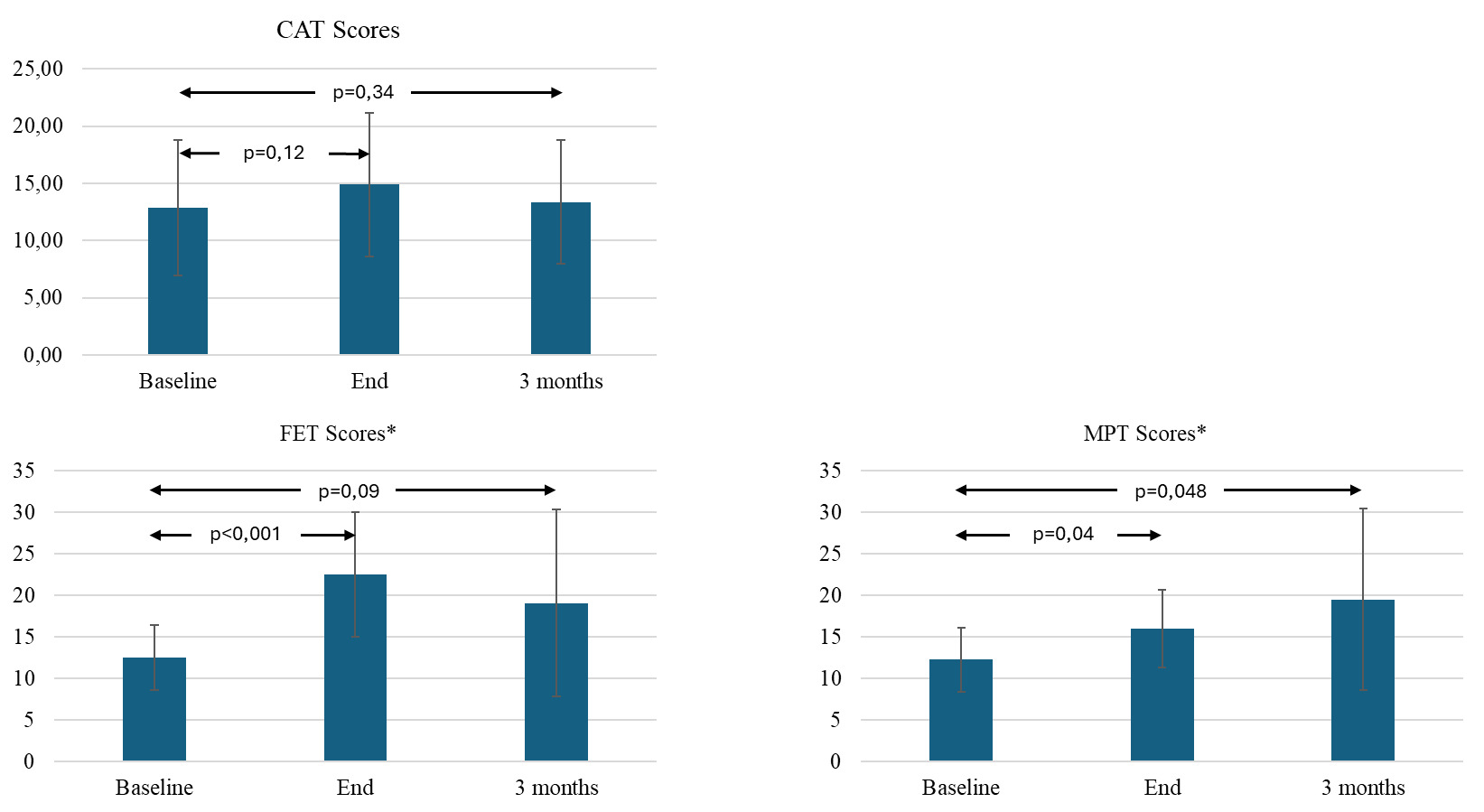
For the CAT scores, there were no statistically significant changes at the end of the intervention (p = 0.115) or at the three-month evaluation (p = 0.342) compared to baseline, showing no change in quality of life in relation to respiratory symptoms. (see Figure 2). For the FET using sustained/s/ production, there was a statistically significant change at the end of the intervention (p < 0.001) compared to baseline. However, this improvement did not seem to be maintained because there was no statistically significant difference between the three-month evaluation and the one at the baseline (p = 0.092). For the MPT using sustained /a/ production, there was a statistically significant change at the end of the intervention (p = 0.041), which indicated an improvement. This seems to be maintained at the three-month time point (T3-T1 p = 0.048).

Participant perceived effect
Participants reported experiencing improvements in their breathing, stating that they felt their breath had become longer and that they had better control over it. They expressed a sense of having increased breath capacity, as one participant noted: “With more breath, you have more energy” (Online-09). Moreover, the in-person participants, who had not previously engaged in PR, felt that they were able to walk longer distances or climb inclines with less effort: “I am able to walk faster and climb slopes more quickly” (In-person-10).
Some participants also reported improvements in speech articulation (or perceived intelligibility) after the intervention: “I now pronounce each word. [it helped me] with my diction” (Online-09). Finally, participants emphasized the emotional benefits of their involvement in the project, stating that singing contributed to greater happiness in their daily lives: “I realize that singing makes me happier” (Online-03).
Mixed results
Comparison of the quantitative and qualitative data revealed convergence and divergence across outcomes. Quantitative measures of respiratory control and social inclusion showed improvement, aligning with participants’ qualitative accounts of better breathing capacity and greater social engagement. This convergence strengthens the interpretation that the program positively impacted these domains.
However, quantitative measures of quality of life did not show improvement. However, the qualitative data diverged from these findings; participants consistently reported feeling happier and more satisfied with their daily lives. This discrepancy suggests that the standardized instruments did not capture perceived improvements in quality of life, demonstrating the added value of qualitative data in documenting meaningful changes.
Discussion
This study explored the experiences of participants in a hybrid GS program that includes in-person and online groups, its effects and perceived effects on respiratory control, quality of life, and social inclusion.
Our qualitative findings further support the role of GS as a socially engaging and psychologically supportive activity. This aligns with previous studies demonstrating that GS is generally well accepted by participants and contributes to their overall well-being.20,45 In our study, the online participation in our hybrid model was valued for reducing infection risk, alleviating performance anxiety, and enabling people to participate even if they lived in different places. The online option allowed participants to join sessions remotely when in-person attendance was not possible, such as during illness. Both in-person and online formats fostered a sense of community. This is consistent with another study, which highlighted that social inclusion is a key component of GS interventions.46 Nevertheless, technological challenges, particularly for online participants, limited opportunities for practice and feedback, which negatively affected engagement and perceived progress.28
The observed increases in FET and MPT in this study suggest improved control during expiration. This improvement likely reflects greater engagement and endurance of the expiratory muscles, as described in singing-related respiratory tasks.23 These findings are consistent with previous studies indicating that structured singing practice can enhance indirect measures of expiratory muscle function in individuals with chronic respiratory disease.25
Additionally, participants perceived the singing-group leader’s competence as enhancing their enjoyment and skill development. This aligns with prior research emphasizing the importance of skilled and engaging leadership in group singing contexts.16,47 However, technological challenges in online or hybrid formats may limit real-time feedback and disrupt session flow. Thus, addressing these barriers is essential to realizing the full benefits of an expert facilitator.
The findings suggest that the participants perceived improvements in respiratory control, quality of life, and social inclusion. These findings were consistent with the quantitative data, except for quality of life. This discrepancy may be explained by the limited sensitivity of the quality of life tools. Also, both in-person and online delivery modes demonstrated positive effects. Consistent with previous studies on in-person GS in COPD populations,18,20 participants reported enhanced breathing control and improved well-being. Importantly, our study adds to the literature by demonstrating that a hybrid format can preserve these benefits while improving accessibility for those facing barriers to attending in-person sessions. This is particularly relevant for individuals with advanced disease, mobility limitations, or concerns about infection risk.
A notable strength of this study is its integration of both qualitative and quantitative methods, allowing for a richer understanding of the intervention’s effects.30 The collaboration with community organizations enhanced recruitment and program delivery, underscoring the potential for partnerships between healthcare and community sectors in long-term disease management. This study is notable for successfully conducting a complex and innovative protocol in a community setting. The study involved multiple partners, a hybrid delivery format and a mixed-methods approach, all of which were achieved with minimal personnel and funding resources.
Limitations
Some limitations should be acknowledged. The broad inclusion criteria resulted in a heterogeneous sample, limiting clinical specificity and generalizability. This variability should be considered when interpreting the findings. However, the variability reflects a community-based, public health approach aimed at promoting equitable access to a low-risk intervention. The one site and absence of a control group limit the transferability of the findings and preclude definitive conclusions about causality. The use of convenience sampling may have introduced selection bias, as participants motivated to engage in group activities may differ from the broader COPD population. Participants in the online group were also participating in a maintenance exercise programme during the GS program, which makes it difficult to distinguish whether the improvement in this group is due to the GS or the exercise program. The reliance on self-reported measures for some outcomes also introduces the possibility of response bias. Also, FET measured using a chronometer and sustained /s/ production represents a functional and approximate indicator of expiratory breath control by reflecting the engagement of the expiratory muscles. It does not provide precise lung function measurements and should not be interpreted as comparable to spirometry, but rather as reflecting expiratory control. Respiratory muscle dysfunction in individuals with chronic respiratory disease is reflected by reduced PEmax.24 Because we chose a more functional measure, FET that reflects expiratory control, improvements in PEmax cannot be assumed, limiting direct comparisons with studies using PEmax. Furthermore, technological barriers were a cause of dropout, suggesting that future implementation efforts should include targeted technical support and training.
Conclusion
This study suggests that hybrid GS can be a socially engaging and psychologically supportive activity for individuals with CRD, offering flexibility in participation while fostering social inclusion. Improvements in respiratory and phonatory endurance were measured and perceived by participants. However, technological barriers, particularly in the online format, can hinder both participant engagement and the group leader’s ability to provide real-time feedback and maintain group cohesion. These findings highlight the need for careful consideration of technological infrastructure, training, and facilitation strategies when designing hybrid or online GS programs. Ensuring competent leadership and a supportive environment remains essential for maximizing the benefits of GS in diverse delivery formats. Future research should include larger, controlled trials to confirm these results, explore long-term adherence, and evaluate the cost-effectiveness of such programs.
Acknowledgments
The authors acknowledge the partnership of SERCOVIE and the manager, Mrs. Annick Beaulé, who offered us general support, such as the venue in their 50+ Community Center, technical equipment and assistance, registration, reception and their Zoom connection; also, the partnership of the QLA and its director, Mrs. Dominique Massie, for promoting the group singing intervention to its members. We were fortunate to have a pianist accompanist for almost all the sessions (Mrs. Céline Lalande) and an experienced chorister/musician for general assistance (Mr. Louis Bureau). We thank the research assistant (Mrs. Solange Nkulikiyinka) for the qualitative interviews and an occupational therapy student (Mr. Jacob Leblanc) for his help with the qualitative analyses.
Research data
Data can be made available through IRB-approved procedures and data sharing agreements to protect participant privacy. For further information on data availability, please contact Dr. Nicole Marquis (nicole.marquis@usherbrooke.ca). The study was not preregistered.
Contributions
All authors contributed to the conception or design of the work, the acquisition, analysis, or interpretation of the data. All authors were involved in drafting and commenting on the paper and have approved the final version.
Ethical approval
The study was approved by the research ethics committee (#2023-4921) of the Centre Intégré Universitaire de Santé et de Services Sociaux de l’Estrie – Centre Hospitalier Universitaire de Santé de Sherbrooke (CIUSSS de l’Estrie – CHUS). Informed consent was obtained from all participants.
Funding
This work was supported by funding from the Toronto Metropolitan University under the Social Sciences and Humanities Research Council (SSHRC) Insight Grants Program SingWell Canada.
Competing interests
All authors have completed the ICMJE uniform disclosure form and declare no conflict of interest.
AI statement
The authors confirm that no generative AI or AI-assisted technology was used to generate content.