Introduction
Patient–Ventilator Asynchronies (PVA) are a frequent phenomenon among patients requiring mechanical ventilation. These events can occur across all modes of mechanical ventilation. An appropriate interaction between the patient and the ventilator is an essential component in reducing associated complications, such as prolonged duration of mechanical ventilation and extended stays in the intensive care unit (ICU).1–5
Currently, a variety of tools are employed in critically ill patients to stratify clinical risk. In the context of mechanical ventilation, several formulas act as indicators of lung injury.6,7 Specifically, in the case of PVA, the Asynchrony Index (AI) has been used to estimate lung damage associated with their occurrence. This index, first proposed in 1997,8 remains the most widely used quantitative method for assessing the quality of patient–ventilator interaction (PVI), establishing a clinical threshold of ≥10%, which is associated with adverse outcomes.9–11
However, recent scientific evidence on ventilatory asynchronies suggests that not all PVAs have the same clinical impact. Some studies have revealed that the extent of injury caused by these events depends on the type of asynchrony, its intensity, and its duration, and that it can be beneficial in some cases.12–15
Consequently, classical AI may present several substantial limitations: in some cases, it may fail to distinguish between the different types of asynchrony, may not account for the duration of exposure to asynchrony events, and may not quantify their intensity or severity.5,12,16,17 These limitations may hinder an adequate characterization of PVI and its potential association with lung injury. In this context, it is necessary to explore more comprehensive and clinically relevant approaches.
Accordingly, the aim of this study is to propose the Asynchrony Index Modified (AIM) as a conceptual and methodological approach intended to address some of the limitations of the traditional AI. This work introduces a theoretical framework and a proof-of-concept model designed to support future research and clinical validation, rather than to establish definitive clinical thresholds or immediate bedside application.
This proposal seeks to offer a more integrative way of describing asynchronies and their potential clinical relevance, while encouraging further investigation into its applicability and impact on the assessment of mechanical ventilation.
Methods
Study design and analytical framework
This study was designed as a methodological and analytical investigation to compare the performance of traditional AI with the proposed AIM. We used both hypothetical simulations and real clinical waveform examples to examine how each index behaves under different asynchrony conditions.
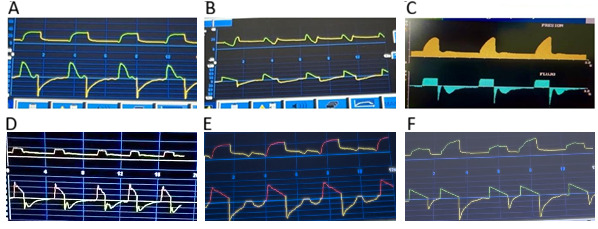
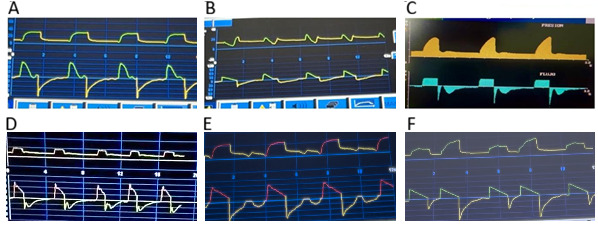
Real ventilatory waveforms were retrospectively selected from routine clinical monitoring in mechanically ventilated patients in the ICU. Cases were chosen to represent six common types of PVA. All ventilatory waveforms were continuously monitored and recorded from modern mechanical ventilators capable of isplaying real-time flow and pressure waveforms.
Formula
Asynchrony Index (AI)
AI=NumberofAsynchronousEventsTotalbreathsx100%
Asynchrony Index Modified (AIM)
The AIM is based on the conceptual premise that PVA is a multidimensional phenomenon rather than a process determined solely by the frequency of events.
Within this framework, three key dimensions are considered essential to characterize this burden: Number of asynchrony events (N), intensity (I), and exposure time (t). Intensity coefficient (I) was incorporated to differentiate the relative clinical importance of the various types of asynchrony. Exposure time (t) was included to capture the temporal dimension of asynchrony, recognizing that sustained exposure—even to less severe events—may generate a clinically significant cumulative effect. To standardize and enable comparison, time was normalized to a reference interval of 60 seconds (T), in line with conventional ventilatory monitoring practices. Normalization by the total number of breaths (B) allows the index to be interpreted in relation to the patient’s ventilatory activity.
These variables were integrated using a weighted multiplicative structure, based on the assumption that the overall burden of asynchrony arises from interactions among its components rather than from their simple summation. According to this model, increases in any individual dimension proportionally amplify the overall effect, consistent with the concept of cumulative physiological stress.
This mathematical formulation was intentionally designed to be simple and clinically interpretable, while providing a quantitative representation.
AIM=(NxIx(tT)BX3)X100%
N: Number of asynchrony events
I: Asynchrony intensity, grouped into three categories
-
Delayed cycling, premature cycling
-
Auto-triggering, excessive flow, insufficient flow, ineffective trigger
-
Double triggering, reverse triggering
t: Exposure/observation time to asynchrony (in seconds)
T: Normalization factor for time (constant, 60 seconds)
B: Total number of breaths
3: Constant normalization factor
%: Expression in percentage
Patient–ventilator asynchrony definitions
Trigger asynchronies were defined as follows: double triggering was defined as two consecutive inspiratory efforts occurring within an interval shorter than half of the mean inspiratory time; auto-triggering as the delivery of a breath that is neither synchronised with the set respiratory rate nor initiated by the patient; ineffective trigger as patient efforts that fail to initiate a ventilatory cycle; and reverse triggering as a ventilator-delivered insufflation that elicits diaphragmatic contraction in response to passive lung inflation.18
Flow asynchronies were defined as insufficient flow, when the delivered gas flow does not meet the patient’s inspiratory demand; and excessive flow, when there is an overdelivery of inspiratory flow in volume-controlled modes or an excessively rapid rise in flow in pressure-controlled modes.19
Cycling asynchronies were defined as premature cycling, when a mismatch exists between neural inspiratory time and ventilator inspiratory time such that the patient’s neural inspiratory time exceeds that of the ventilator; and delayed cycling, when the opposite occurs, namely when ventilator inspiratory time exceeds the patient’s neural inspiratory time.19
Ethical considerations
Formal research ethics approval was not required for this study, as it was based on simulated cases and methodological modelling. The ventilatory waveforms used were derived from routine clinical monitoring and did not involve any modification of treatment or clinical management.
Statistical analysis
Given the conceptual and proof-of-concept nature of this study, no inferential statistical analyses were performed. The analysis was limited to descriptive comparisons between the AI and the AIM in simulated and representative clinical scenarios, using predefined and standardized equations for each index.
The results were expressed as percentages and analyzed to illustrate how each index responds to controlled changes in these variables.
This approach was chosen to emphasize the theoretical performance and discriminatory capacity of the AIM model, rather than to establish statistical significance or population-level inferences.
Results
To facilitate the presentation, the following section includes illustrative examples based on both hypothetical scenarios and representative clinical waveforms, allowing a structured comparison across different asynchrony conditions.
For illustrative purposes, a hypothetical example is presented in which two observation periods are compared, each with different exposure times to asynchrony events and distinct types of PVA. In both scenarios, N = 8 asynchrony events and B = 15 total breaths were recorded, with T = 60 seconds, varying only in the exposure time and the type of asynchrony (see Table 1).
Under these controlled conditions, the AI remained unchanged (53.33%) across all scenarios, as it depends solely on event frequency. In contrast, the AIM increased proportionally with both longer exposure times and higher intensity levels.
This comparison illustrates that, unlike the AI, the AIM appears to be capable of discriminating between clinically distinct scenarios that share the same number of asynchrony events but differ in their temporal persistence and physiological severity. Therefore, AIM provides additional information on the cumulative burden of asynchrony that is not captured by frequency-based indices alone.
Representative ventilatory waveforms illustrating six types of PVA are shown in Figure 1, with the analysis shown in Table 2.
Discussion
In the field of intensive care, continuous knowledge updating is essential, and clinical tools must evolve in parallel with scientific understanding.20,21 The AIM was developed in response to recent advances in the understanding of PVA, incorporating dimensions that were previously overlooked in traditional assessments.
To our knowledge, the AIM may represent one of the first proposed indices integrating frequency, intensity, and duration of PVA into a single quantitative metric. The results of this study help to explain the implications of this approach. While the AI yielded identical values across scenarios with the same number of events, the AIM was able to differentiate between conditions with varying exposure times and levels of asynchrony severity. This suggests that the AIM could capture dimensions of PVI that are not reflected in traditional frequency-based measurements. By incorporating both the temporal persistence and physiological impact of asynchrony events, the AIM may provide a more comprehensive estimation of the true clinical burden of patient–ventilator mismatch.
For decades, PVI has been predominantly assessed using the traditional AI,8 a frequency-based metric that quantifies the proportion of asynchronous events relative to total breaths. Although this approach was valuable at the time of its introduction, its limitations have become increasingly apparent in the context of modern critical care, where patients exhibit complex and dynamic respiratory patterns.22,23 Specifically, the AI does not differentiate between types of asynchronies, nor does it account for the duration of exposure or the intensity of patient–ventilator uncoupling. Consequently, it may oversimplify the clinical relevance of PVA and obscure physiologically meaningful distinctions.
Recent experimental and clinical studies support the notion that not all asynchronies exert equivalent effects on the respiratory system. For instance, Damian et al.24 demonstrated that reverse triggering during lung-protective ventilation may contribute to diaphragm dysfunction, highlighting that specific asynchrony patterns can have distinct and potentially harmful physiological consequences that are not captured by frequency-based indices alone. Similarly, Brito et al.25 reported that double triggering with breath stacking may sometimes reflect intrinsic respiratory variability rather than uniformly injurious mechanical interaction, further illustrating the heterogeneity of PVA.
Moreover, emerging evidence regarding variations in respiratory drive and muscle effort reinforces the inadequacy of purely event-counting metrics. Indices that fail to consider effort magnitude risk underestimating potential ventilator-induced injury in patients with high respiratory drive, while potentially overestimating harm in those with low effort. These observations underscore the need for a more nuanced and physiologically informed assessment tool.26
In this study, comparison between AI and AIM demonstrated that, while the traditional AI remains static when the number of asynchronies and breaths is unchanged, the AIM varies proportionally with both exposure time and asynchrony intensity. This behaviour suggests that the AIM the AIM could be more sensitive to clinically relevant differences in PVI and may better reflect the true asynchrony burden. Notably, in our hypothetical scenarios, two patients with identical AI values would present markedly different AIM scores depending on asynchrony characteristics, illustrating a key limitation of the traditional index.27,28
Similarly, analysis of real clinical cases revealed that the AI remained constant at 100% across different types of PVA, whereas the AIM discriminated between delayed cycling, insufficient flow, and reverse triggering. This finding supports the clinical utility of the AIM as a conceptual tool capable of capturing meaningful differences in ventilatory interaction that are otherwise masked by conventional metrics.
The clinical relevance of this approach is further supported by experimental work from Hashimoto et al.,29 who showed that distinct forms of asynchrony produce different patterns of tissue injury. Breath stacking was associated with more severe lung injury and impaired oxygenation, whereas reverse triggering primarily affected diaphragmatic function. These results reinforce the premise that the type and intensity of asynchrony rather than its mere frequency are critical determinants of clinical impact.
From a broader perspective, the increasing emphasis on precision and personalized strategies in critical care demands assessment tools that reflect physiological complexity.30 As highlighted by de Wittenstein et al.31 PVI is a highly dynamic process that cannot be adequately characterized by overly simplistic indices. In this context, the AIM could represent not only a new formula but a conceptual shift in how ventilatory quality is evaluated.
Importantly, the AIM is designed to be practical and easily integrated into routine clinical practice. It requires no additional technology, relying instead on standard ventilator waveforms and structured analysis of asynchrony characteristics. This feature enhances its feasibility for bedside implementation in diverse clinical settings.
Limitations
This study has limitations; most notably, a validated clinical threshold for the AIM has yet to be established. However, the primary objective of this work was to propose and justify a novel integrative framework rather than to define definitive cutoff values. Future prospective studies could evaluate the association between AIM values and clinical outcomes, enabling the development of evidence-based reference ranges tailored to different asynchrony intensities and patient populations. Additionally, further work is needed to refine the intensity classification system and explore whether alternative weighting strategies might enhance the predictive performance of the AIM.
Conclusion
The AIM may represent a promising approach for the assessment of PVI. By incorporating dimensions such as asynchrony type, intensity, and duration of exposure, it seeks to address some of the limitations of the traditional AI and to offer a more comprehensive and physiologically informed description of ventilatory synchrony. Rather than treating all asynchronies as equivalent events, the AIM may help to better characterize the burden of patient–ventilator mismatch, potentially allowing for a more nuanced interpretation of its clinical implications.
This proposed index provides a theoretical framework for future research and may contribute to ongoing efforts toward more individualized approaches to mechanical ventilation in critical care. However, these findings are based on a theoretical framework and a proof-of-concept model, and further studies are required to evaluate its clinical applicability, validity, and potential impact before considering its use in routine practice.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
All authors have completed the ICMJE uniform disclosure form and declare no conflict of interest.
Ethical approval
Formal research ethics approval was not required for this study, as it was based on simulated cases and methodological modelling.
AI Statement
The authors confirm no generative AI or AI-assisted technology was used to generate content.