

Introduction
Acute respiratory distress syndrome, or ARDS, is an important complication of COVID-191 and one of the main reasons for ICU admission of patients afflicted with the illness. ARDS is a life-threatening lung condition that is characterized by extensive inflammation, lung damage, and pulmonary edema, which lower oxygen levels and cause breathing difficulties.2 Some evidence has questioned whether COVID-19-associated ARDS (CARDS) and typical ARDS are truly different,3–5 despite many clinical characteristics appearing similar to those of the “non-COVID-19” ARDS.6–9 The potential distinguishing features of SARS-CoV-2-induced ARDS and suggested management strategies for patients with severe COVID-19 are hotly contested topics.10,11 One reason for the controversy is the variability of clinical characteristics among COVID-19 patients with ARDS. The two phenotypes of CARDS are typical ARDS (“H-type”), which is characterized by reduced lung volume, decreased lung compliance, and unmatched ventilation-perfusion ratio, and a distinct condition known as “silent hypoxia,” which is linked to nearly normal lung compliance and progressive respiratory distress.12 Another one is its distinct pathophysiology,13,14 which may alter current evidence-based management strategies for CARDS.15–19
Glucocorticoids are used to reduce mortality in patients with CARDS who are admitted to ICU20; nonetheless, there are substantial problems with their accurate clinical treatment and survival.21,22 Furthermore, when the COVID-19 pandemic began, CARDS patients were also treated with antiretrovirals like lopinavir and ritonavir in compliance with the WHO guidelines. However, these guidelines were adjusted as more information about their safety and efficacy was available. In this investigation, we particularly concentrated on non-pharmacological approaches to address ARDS. At a glance, literature searches yield results that are partly conflicting regarding the precise clinical management of CARDS patients admitted to ICU.4,6,23–26 Therefore, the purpose of this study was to use advanced data mining techniques in conjunction with survival analysis to do a retrospective, observational analysis of the clinically relevant parameters impacting the survival of CARDS to ICU compared to non-COVID-19, other-etiology ARDS patients.
Methods
Selection and classification of COVID-19 and non-COVID-19 ARDS cases
Data from patients’ electronic medical records of the Guasmo Sur General Hospital (Guayaquil, ECUADOR) were collected and reviewed by physicians trained in critical care. The study comprised 1,341 consecutive patients with low-to-moderate and severe ARDS (i.e., alveolar pressure / inspired oxygen fraction (PaFi) less than 300) admitted in the ICU from February 2020 to August 2022. The Berlin definition2 was used to diagnose ARDS as the primary reason for ICU admission. ARDS-ill patients were included in either the CARDS cohort (patients with a positive RT-qPCR test for SARS-CoV-2) or in the typical ARDS cohort (patients with a negative RT-qPCR test for SARS-CoV-2) based on the CDC 2019-Novel Coronavirus Real-Time RT-PCR Diagnostic Panel in upper and lower respiratory specimens. Approximately 95% of the patients received corticoid treatment.
Data processing and feature selection
A dataset containing a variety of clinical variables and outcomes was obtained from the hospital’s digital records. The initial step in data processing entailed performing an exploratory analysis to determine the various data categories, the COVID-19 patient’s status of discharge, and a distribution of features (a comprehensive list is supplied in Supplementary Material 1). Further processing addressed missing values via imputation (if any), scaled the numerical variables, and encoded the categorical features to ensure interoperability with the machine learning techniques implemented in Python programming language.27
Statistics
Statistical analysis of the data was performed using Rstudio free software environment (https://www.r-project.org/). While Welch’s t-test was used to evaluate quantitative data (given as mean ± SD), the Chi-square test was utilized to analyze categorical data. The multivariable Cox proportional hazards regression models with the enter method were used to evaluate the relationship between risk factors and ICU mortality. The Kaplan-Meier survival estimates and the log-rank test were used to analyze sex-and age-dependent effects in terms of survival. Alpha threshold was always set at 0.05.
Ethics
On December 4th, 2023, the Manabí Tech University Ethics Committee approved this study (Ref# CEISH_UTM_EXT_23-11-29_SJB), and each subject provided written informed consent. The ICU medical director at the Guasmo Sur General Hospital gave the authorization to download the information from the digital clinical records system. The Declaration of Helsinki was followed when conducting the study.
Results
Nature and distribution of the sample
A total of 1,340 cases of ARDS patients were in intensive care; 716 male patients (53.43%) and 624 female patients (46.57%) were included. After that, the sample was split into two cohorts: the non-COVID-19 ARDS cohort (332 ARDS cases including 158 males (47.59%) and 174 females (52.41%)) and the COVID-19-associated ARDS cohort (1008 CARDS patients including 558 males (55.36%) and 450 females (44.64%)). The primary causes of ARDS that were not associated with COVID-19 were septic shock (20.5%), obstetric emergencies (14.7%), abdominal trauma (11.7%), pneumonia (10.3%), and pancreatitis (4.4%). Compared to normal ARDS cases (n= 91, 27.41%) (χ2= 7.26, p < 0.01), the death rate among CARDS cases (n= 508, 50.40%) was substantially greater. More men (n= 293, 57.68%) died in the CARDS cohort at a higher rate than women (n= 215, 42.32%), but the differences were not statistically significant (χ2= 2.05, p= 0.153). Males (n= 54, 59.34%) were considerably more affected by mortality in the ARDS group than females (n= 37, 40.66%) (χ2= 6.31, p < 0.05). Patients with CARDS and ARDS had averaged ages of 54.1 ± 15.26 years and 41.06 ± 18.11 years, respectively. In both the ARDS cohort (survivors: 38.19 ± 17.22 years and non-survivors: 48.67 ± 18.30 years; t(153)= -4.73, p < 0.001) and the CARDS cohort (survivors: 49.6 ± 15.33 years and non-survivors: 58.53 ± 13.83 years; t(992)= -9.70, p < 0.001), the death rate rose with age.
Feature selection
The evaluation metrics of the algorithms when classifying patient’s survival are shown in Table 1. Despite slight overfitting, the tuned Random Forest model proved to be the most effective across most metrics in predicting mortality in ARDS patients submitted to intensive care, showing a training and test precision of 98% and 86%, respectively. A Random Forest model for feature selection and dimensionality reduction helped identify crucial predictors for ICU mortality, including mechanical ventilation-related factors (FiO2, PaO2/FiO2), pO2, age, superinfection, shock, blood pH, and ICU length of stay (Figure 1).

Survival analysis and associated risk factors
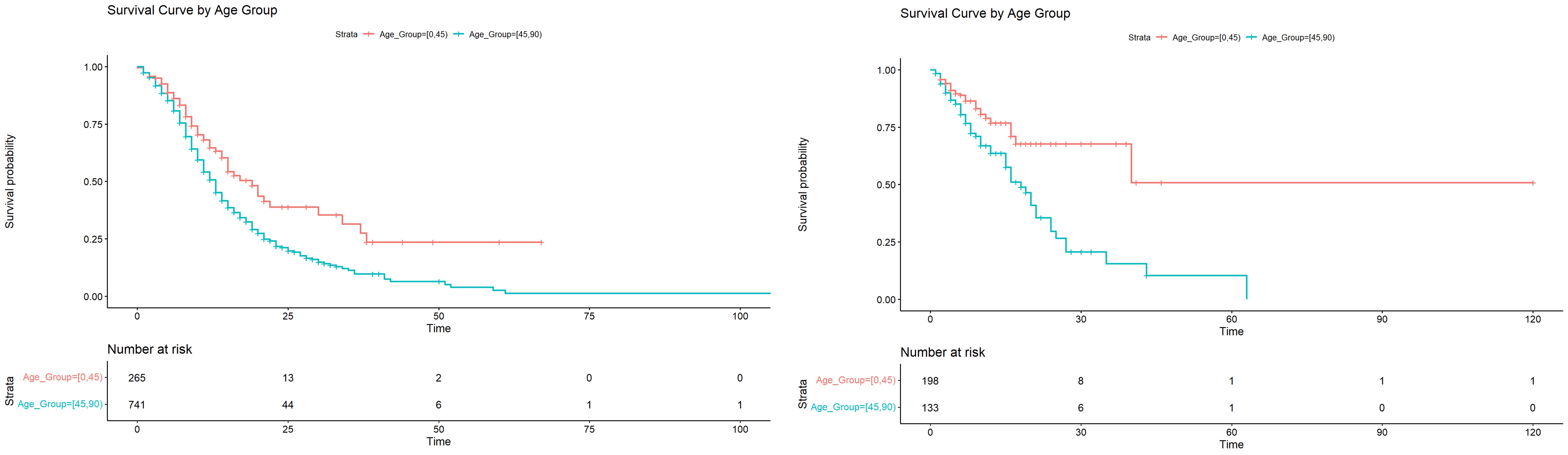
Risk factors for mortality due to the ICU length of stay were separately analyzed in CARDS and ARDS cohorts using the Cox proportional hazards regression model. Table 2 together shows the outcomes of the Cox multivariate analysis in CARDS and ARDS cohorts. Even if most variables were statistically associated with mortality during the ICU stay, their hazard ratios were close to 1 and, therefore, irrelevant from a clinical perspective. Risk factors affecting ICU survival varied across CARDS and ARDS cohorts. On the one hand, high-flow nasal cannula (t= -6.57, p < 0.001)) and reintubation (t= -4.2, p < 0.001) significantly increased ICU survival of CARDS patients. On the other hand, mechanical ventilation (t= 3.36, p < 0.001) and superinfection (t= 2.90, p < 0.001) were significantly associated with the premature death of ARDS patients during their ICU stay (Table 2). Survival showed sex-dependent differences only in the ARDS cohort. Women with ARDS had a lower average risk for mortality due to the ICU length of stay compared to their male counterparts (χ2=6.31; p < 0.01) (Figure 2). Regarding the influence of age (Figure 3), as expected, patients over 45 years old had less chance of surviving an ICU stay (CARDS group: χ2=68.53; p < 0.0001; ARDS group: χ2=22.62; p < 0.001).
_and_ards_(right).jpg)
_and_ards_(right).jpg)
Discussion
The key finding of this study was that, in both cohorts, the management of ARDS with respiratory treatments had a varied impact on ICU survival. The CARDS cohort’s survival was greatly dependent on the delivery of a high-flow nasal cannula and reintubation in particular. Due to the length of ICU stay, mechanical ventilation and consequent superinfections were risk factors for death in the typical ARDS cohort.
Volume-Controlled Ventilation (VCV) and Pressure-Controlled Ventilation (PCV) were the most commonly utilized ventilator modes for treating CARDS and ARDS, respectively, based on our database. These modes make it possible to precisely modify respiratory parameters, which helps with lung protection and ventilator management. Furthermore, non-traditional modes, including Airway Pressure Release Ventilation (APRV) and Pressure-Regulated Volume Control (PRVC), were used, showing effectiveness in minimizing ventilator-induced lung damage and optimizing oxygenation. By lowering alveolar distension pressure and raising the ventilation-perfusion ratio, these non-conventional methods hoped to increase survival rates and lessen pulmonary consequences in ARDS patients.28
Our database also showed that different approaches were used to manage Positive End Expiratory pressure (PEEP) titration and alveolar recruitment. An inflation-deflation index was performed before alveolar recruitment maneuvers (ARM) to evaluate the lung’s resistance to pressure fluctuations and ascertain the maneuver’s efficacy. Particular methods for recruiting alveoli were used, such as ARM, which involves temporarily raising airway pressure to expand collapsed alveoli—furthermore, PEEP changes based on the patient’s hemodynamic response and oxygenation. By reducing the danger of barotrauma and volutrauma and maximizing the benefits of alveolar recruitment, these measures were intended to improve lung protection and survival in patients with ADRS.28 The patient was successfully managing spontaneous ventilation when specific criteria were fulfilled, such as PEEP equal to or less than 5 cmH20 and FiO2 equal to or less than 0.4. This allowed for the gradual reduction or withdrawal of mechanical breathing.
Using machine learning technologies made it possible to identify the most pertinent clinical features for ARDS patients requiring intensive care to forecast their mortality.29 For example, the use of mechanical ventilation could increase the chance of superinfection-related death, which resulted in a decrease in the survival of the ARDS group during their ICU stay.30 Remarkably, ventilator strategies related to the clinical handling of respiratory insufficiency, such as oxygenation through high-flow nasal cannula and frequent intubations, were selected for the ICU survival in the CARDS cohort,16,18,20,21 rather than the most commonly used organ dysfunction scales, such as SOFA31 and APACHE II.32 According to Grieco et al. (2020),33 the explanation could be the respiratory system’s compliance, which differs between CARDS and more conventional ARDS.14,15 Normalization of the early disparities in pulmonary compliance, following sufficient oxygenation and ventilator control, might be crucial for CARDS patients’ survival during their ICU stay.34 Respiratory failure is the most common cause for re-intubation and worse outcomes in CARDS patients.35 Although re-intubation may be independently linked to CARDS mortality,36 our data showed that it increased survival to ICU in CARDS patients. Consistent with earlier research, the high-flow nasal cannula (HFNC) was a crucial factor in treating moderate-to-severe CARDS, as it helped reduce mortality in these patients.37 This oxygenation device offers a high flow of humidified air through a nasal cannula, greatly increasing oxygenation and reducing respiratory effort compared to mask ventilation or conventional oxygen therapy.
In addition to HFNC and re-intubation, medication may also impact CARDS. While quick results to confirm the existence of COVID-19 were not available, dexamethasone was chosen as the standard treatment for ARDS of non-infectious etiology to minimize patients’ pulmonary inflammation and improve respiratory function. The ROX index was used to evaluate the monitoring and efficacy of the HFNC system. Interestingly, corticosteroids and HFNC worked well together to control ARDS and improve patient survival, which led to a notable drop in the illness-related death rate. Antivirals probably had a limited impact because they were only prescribed to CARDS patients, too, right at the start of the pandemic.
Different underlying factors can induce ARDS, which is not connected with COVID-19.1 One of the main causes is pneumonia, which frequently results in primary ARDS and causes significant inflammation and destruction of the alveoli. Another important factor is trauma, especially abdominal trauma, which can result in a systemic inflammatory response that affects the lungs. Septic shock, a condition in which sepsis and extensive infection cause multiple organ failure, including the lungs, is another important component. Due to a confluence of hemodynamic and inflammatory variables, obstetric emergencies such as severe preeclampsia, amniotic fluid embolism, and postpartum hemorrhage can cause ARDS. Finally, severe secondary inflammation leading to ARDS can be caused by acute pancreatitis due to the production of inflammatory cytokines and pancreatic enzymes. Our database showed that these causes matched the trends found in cases of recorded ARDS, demonstrating the variety and complexity of etiological elements.
In light of everything mentioned above, CARDS and ARDS may not fully respond to the same standard ventilation techniques,14,38,39 even though there may be some similarities in the respiratory mechanics of both conditions.40–42 Additionally, the data indicated that SARS-CoV-2 infection led to worse outcomes, consistent with previous research5,7 but inconsistent with other studies.9 In addition to the greater age of our CARDS sample, variations in survival over an ICU stay may be explained by minor physio-pathological changes between CARDS and ARDS that would impact respiratory efficiency.43–47 Finally, the results of our investigation agree with previous research in that although hospitalized women have a lower risk of dying from COVID-19, once they are admitted to the ICU, their risk of death is comparable to that of men48 (Figure 2). Age was a risk factor for ICU mortality in both cohorts (Figure 3), as previously reported.49
Although the retrospective approach and the review of records from a single institution could be seen as drawbacks, the study showed a substantial sample of patients from a COVID-19 reference hospital in Guayaquil, the largest city on Ecuador’s coast. Ecuador declared Guayaquil its pandemic zero zone. During the COVID-19 outbreak, Ecuador had the highest death toll in all of South America.
Conclusion
In summary, our results provide insight into specific evidence-based respiratory therapy (high-flow nasal cannula and re-intubation) for CARDS patients, for whom there are now only supportive ICU care choices available (with the exception of corticoid administration). Further research is needed to support the adjustment of ventilator and oxygenation settings in CARDS cases.
Acknowledgements
We are grateful to the health professionals of the Hospital General Guasmo Sur in Guayaquil (Ecuador), who treated the patients and worked with us in the management of the database. We would especially like to thank Jazmin Gallego-Polo.
Authorship Contributions
Paulo Navas-Boada was responsible for the conceptualization of the work and the resources. Kevin Chamorro made significant contributions to data curation, formal analysis, and validation. Santiago Ballaz was in charge of supervision and the writing of the original draft. All authors equally contributed to writing, review, and editing of the final manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare there is no conflict of interest.
Ethical Approval
The Manabí Tech University Ethics Committee approved this study (Ref# CEISH_UTM_EXT_23-11-29_SJB).
Data availability
The datasets generated analyzed during the current study are available from the corresponding author on reasonable request.
AI Statement
The authors confirm no generative AI or AI-assisted technology was used to generate content.