Introduction
SARS-CoV-2 develops a respiratory disease with systemic involvement.1 Severity of the disease is variable; in a Chinese study with 72314 cases2 including outpatients and patients admitted to hospital, 14% had severe pneumonia, and 5% were critical cases. Also, another Chinese study1 reported that 15-20% of the inpatients required ventilatory support. Overall mortality has been reported from 21 to 28% in hospitalized patients,3,4 and it rises to 61.5 to 62% in patients in an Intensive Care Unit (ICU)4,5
Patients with chronic lung diseases (CLD), particularly chronic obstructive pulmonary disease (COPD) and asthma, would be expected to be at increased risk of SARS-COV-2 infection and more severe COVID-19 course.6–12 However, none of these diseases are main comorbidities in patients with COVID-19.6,13 Only 0.95% - 5.1% of admitted patients with COVID-19 had a CLD.14,15 A study reported a lower risk of hospital admission for COVID-19 in patients with COPD and asthma.16
It has been hypothesized that chronic inhaled corticosteroids (ICS) could affect the development of SARS-COV-2 infection.6,15 In patients with COPD and asthma, ICS has been associated with an increased risk of upper respiratory infections, and ICS has been associated with a higher prevalence of pneumonia.17 Furthermore, in-vitro models suggest that ICS could delay virus clearance.17 In contrast, ICS alone or in combination with bronchodilators has been shown to suppress coronavirus replication and cytokine production in HCoV-229 coronavirus infection in in-vitro models.18 Moreover, ciclesonide suppresses viral replication of SARS-COV-2 in-vitro, ICS downregulates the SARS-COV-2 receptor ACE2 in-vitro in COPD patients, and long-term use of inhaled corticosteroids for controlling asthma is likely to have a beneficial modulatory effect on COVID-19.19–21
Taking into account the contradictory data on the possible benefits6,14–16,18–21 or harms6,17 of inhaled corticosteroids (which are administered worldwide to the majority of asthmatic and COPD patients16) on the prognosis of COVID-19, we have carried out this study to investigate the influence that chronic ICS may have on the prognosis of COVID-19 hospitalized patients with CLD.
Methods
Study design and participants
This is a multicenter retrospective cohort study of patients with SARS-CoV2 infection, aged ≥18 years, who were hospitalized between March and September 2020 in Spain and included in the SEMI-COVID-19 Network.3 The registry is an initiative of the Spanish Society of Internal Medicine (SEMI, for its initials in Spanish), which included 17,416 cases by September 2020, and its characteristics have been described elsewhere.3,12 Data are collected retrospectively and include epidemiological and clinical characteristics, such as comorbidities, symptoms, physical examination findings, laboratory and diagnostic imaging test results, and clinical outcomes. STROBE Statement Guidelines were followed in the study’s design and reporting.
Definitions and data source
COVID-19 was defined as compatible symptoms and a positive result on either polymerase chain reaction (PCR) of a nasopharyngeal sample or serology test for SARS-CoV-2. Chronic lung disease (CLD) was defined as an antecedent of COPD or asthma diagnosticated by pulmonary function tests or clinical criteria of chronic bronchitis. Clinical criteria of chronic bronchitis is clinically characterized by a persistent cough lasting at least three months over two or more consecutive years.22 These changes significantly impair lung compliance and pulmonary function.23,24 Chronic bronchitis is associated with a diminished quality of life, a more rapid decline in lung function, increased frequency of exacerbations, and a higher risk of mortality, as highlighted in research by Kim et al. in 2016 and 202.25,26 Pulmonary function tests are used in the evaluation, classification and grading of a variety of forms of lung diseases with the performance of basic spirometry with or without other additional tests such as spirometry before and after a bronchodilator, lung volumes and quantification of carbon monoxide diffusing capacity. Chronic ICS use was retrieved from electronic medical records. Patients with a long-term prescription written in the past 12 months were included. Fever was considered as an axillary temperature of 38ºC or more.3
Outcome measures
The primary outcome of this study was in-hospital mortality. Secondary outcomes were the development of moderate-severe Acute Respiratory Distress Syndrome (ARDS) according to the Berlin 2012 criteria,27 transfer to an ICU, requirement of invasive mechanical ventilation, and length of stay (LOS).
The increase of inflammatory parameters (c-reactive protein, ferritin, interleukin 6, D-Dimer, lymphocyte, lactate dehydrogenase and fibrinogen) were also analyzed, comparing their values at admission and on day +7 of hospitalization and comparing the difference of medians.
Statistical analysis
Continuous variables were expressed by mean, standard deviation (SD) or median, and interquartile range (IQR). Categorical variables were summarized in terms of frequencies and percentages. Differences between groups were determined using the chi-square test or Fisher’s exact test for categorical variables; the Mann-Whitney U test, Student’s t-test or analysis of variance were used for continuous variables, as appropriate. P values <0.05 were considered statistically significant. Cases with missing data were excluded from the analysis. The SPSS statistical package version 22.0 (SPSS, Chicago, IL) was used.
Ethical aspects
Scientific and ethical permission to conduct this study was obtained from the Provincial Research Ethics Committee of Málaga (Spain). Personal data were processed in strict compliance with Spanish Law 14/2007 on Biomedical Research; Regulation (EU) 2016/679 of the European Parliament and of the Council of April 2016 on the protection of natural persons concerning the processing of personal data and on the free movement of such data (General Data Protection Regulation); and Spanish Organic Law 3/2018 on Personal Data Protection and the Guarantee of Digital Rights.
Results
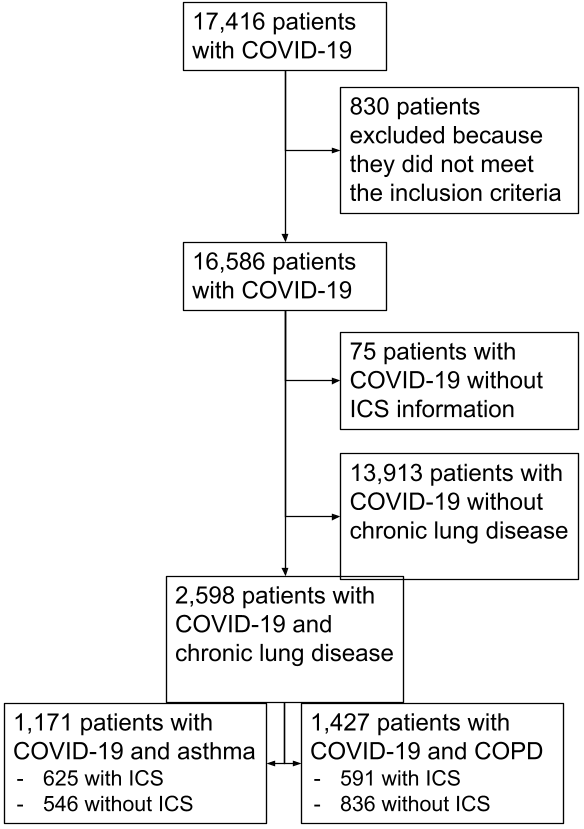
Of the 17,416 patients included in the SEMI-COVID Network by September 2020, 2,598 patients had CLD, of which 1,171 patients had a diagnosis of asthma and 1,427 of COPD (see Figure 1). The mean age was 76.7 years (IQR 69.7-83.9) in COPD patients and 65.6 years (IQR 52.6-76.8) in patients with asthma. Both asthma patients with ICS and COPD patients with ICS had a significantly higher mean age [(asthma patients: 66.6 years vs. 63.4 years, p < 0.001), (COPD patients: 77.5 years vs. 76.6 years, p = 0.009)]. 79.1% of COPD patients were male, and 40.2% of asthma patients were male. Most of the patients (66.8% asthma patients and 94.5% COPD patients) had an adjusted Charlson Comorbidity Index of 3 or more points, being more frequent in those with ICS [(72.2% vs. 60.6%, p < 0.001 in asthma patients); (96.1% vs. 93.3%, p = 0.025 in COPD patients)]. The most frequent comorbidities in asthma patients were hypertension (47.4%), diabetes (15%) and heart failure (6.7%). In comparison, the most frequent comorbidities in COPD patients were hypertension (67.6%), cancer (31.6%) and diabetes (28.2%). In COPD patients, the severity of the condition was assessed with FEV1. As may be expected, patients with ICS had a more severe COPD. Other epidemiological characteristics of the patients may be seen in Table 1.

The most frequent symptoms in chronic respiratory patients triggered by the COVID-19 infection were dyspnea (70.9% and 71.3% in asthma and COPD patients, respectively), fever (62.4% in asthma patients and 52.9% in COPD patients) and dry cough (59.9% in asthma patients and 48.5% in COPD patients). Dry cough was significantly more frequent in patients without ICS [(59.4% vs. 60.6%, p = 0.001 in asthma patients), (45.2% vs. 50.8%, p = 0.006 in COPD patients)]. In comparison, productive cough was significantly more frequent in patients with ICS [(23.1% vs. 15.6%, p < 0.001 in asthma patients), (29.6% vs. 22.2%, p = 0.006 in COPD patients)]. Dyspnea was more frequent in patients with ICS, being statistically significant in COPD patients (76.1% vs. 67.9%, p = 0.001). At lung auscultation, wheezing and roncus were more frequent in both asthma and COPD patients with ICS. Other clinical data are shown in Table 2.
Regarding the inflammatory parameters (Table 3), there was a significant decrease in CRP and IL6 in all groups, except in COPD patients with ICS, where the decrease was not statistically significant (p = 0.087). Ferritin increased in all groups but was statistically significant only in COPD patients (with ICS p = 0.001, without ICS p = 0.003). D-dimer also increased in all groups but was not statistically significant in COPD patients with ICS (p = 0.062). Lymphocytes increased in asthma patients (statistically significant in asthma patients with ICS, p = 0.041) and decreased in COPD patients (statistically significant in COPD patients without ICS, p = 0.045).
Patients with chronic ICS had a longer hospital stay in asthma and COPD patients (9 vs. 8 days, p = 0.031 in asthma patients), (11 vs. 9 days, p = 0.018 in COPD patients). No differences were found in-hospital mortality, transfer to ICU, or the development of moderate-severe ARDS (Table 4).
Discussion
In our study, we aimed to investigate the influence of chronic treatment with ICS on the prognosis of COVID-19 hospitalized patients with CLD. We found that patients with COVID-19 and chronic ICS did have more dyspnea and productive cough at admission, as well as a longer hospital stay. Chronic treatment with ICS in patients with asthma and COPD did not influence in-hospital mortality or other prognostic factors such as transfer to ICU, development of moderate-severe ARDS or requirement of invasive mechanical ventilation.
At the beginning of the SARS-CoV-2 pandemic, it was suggested that patients with CLD could have a worse prognosis.11 Influence of chronic ICS was controversial since its use is a known risk factor for pneumonia,28,29 but it was also suggested that it may improve prognosis due to its inhibition of viral replication.19 The STOIC and PRINCIPLE trials published later showed that inhaled budesonide in outpatients reduced time to recovery after early COVID-19, and a recently published clinical trial suggests that using inhaled budesonide may reduce the risk of worsening in hospitalized patients with COVID-19 pneumonia.30,31
In our results, patients treated with chronic corticosteroid therapy (both asthma and COPD) had a higher mean age and more comorbidities, just as was inferred in other articles, compared to patients without ICS. Patients with CLD treated with chronic ICS did not have more severe disease at admission, according to qSOFA and CURB-65, despite having more comorbidities (Charlson ≥3 83.8%). In addition, the severity of COPD (assessed with FEV1) was associated with an increased use of inhaled corticosteroids, as expected.32,33
Asthma and COPD patients treated with chronic ICS did not have higher in-hospital mortality, coinciding with other studies,17,29,34 nor had higher rates of moderate-severe ARDS, transfer to ICU or requirement of invasive mechanical ventilation. Similar results were found by Sen P. et al. in patients with COPD who tested positive for COVID-19.35 However, both asthma and COPD patients treated with ICS had a longer hospital stay. The fact that these patients had a longer hospital stay could be due to factors such as older age and comorbidity measured with the Charlson comorbidity index.
In our study, patients with CLD treated with chronic ICS had a more frequently productive cough, as suggested by Hasan et al. in a study that associates ICS with the risk of respiratory infection.28
It has been suggested that chronic ICS may reduce the inflammation produced by SARS-CoV-2.17,19,21 We analyzed the evolution of inflammatory parameters of these patients during admission and observed that chronic ICS did not have an influence. To our knowledge, this is the first multicenter study that evaluates the evolution of these parameters, which have been related to poor prognosis in COVID-19,36 in patients with chronic ICS.
The main strength of this study is its multicenter, nationwide design and the large number of patients included. The main limitation is that only inpatients were included; therefore, the results may be different for outpatients. Another important limitation is that the different types of ICS were not analyzed separately, so their different degrees of systemic effects could influence the results. Because of the study’s retrospective design, some patients had incomplete information regarding their use of inhaled corticosteroids; these patients were not included, as described in the flow chart (Figure 1). It should be taken into account that the study was developed during the first and second waves of COVID-19 in Spain with different strains of SARS-CoV-2 than from those currently existing and without any vaccination.
The outcomes of this study support the maintenance of ICS in patients admitted for COVID-19. Despite its limitations, its results are very useful in clinical practice since the patients in this study have epidemiological characteristics similar to those in subsequent pandemic waves.37
Conclusions
Patients with chronic inhaled corticosteroids had longer hospital stay and more chronic comorbidities, measured by the Charlson comorbidity index, but they did not have more severe disease at admission, evaluated with qSOFA and PSI scores. Chronic treatment with ICS had no influence on the prognosis of patients with chronic lung disease and COVID-19.
Acknowledgments
We gratefully acknowledge all the investigators who participated in the SEMI-COVID-19 Registry.
Funding
This research has not received specific support from public sector agencies, the commercial sector or non-profit entities.
Ethical Approval
Scientific and ethical permission to conduct this study was obtained from the Provincial Research Ethics Committee of Málaga (Spain).
Competing Interests
All authors have completed the ICMJE uniform disclosure form and declare no conflict of interest.
AI statement
The authors confirm no generative AI or AI-assisted technology was used to generate content.